A Plague Upon Our House: My Fight at the Trump White House to Stop COVID from Destroying America
Scott W. Atlas, M.D.
Post Hill Press, New York, 2021
A Plague Upon Our House is Scott Atlas’s personal account of his four months (“end of July” 2020 — December 1, 2020) as a special adviser to the White House on the COVID-19 pandemic and pandemic response. It also discusses some of his interactions with and advice to Florida state governor Ron De Santis. The book paints an alarming picture of key medical advisers Tony Fauci, Deborah Birx, and Robert Redfield as incompetent, highly political, dishonest career bureaucrats in the worst sense of the words and President Trump as a disengaged, indecisive, publicity obsessed leader quite far from his abrasive, tough, “You’re fired!” public image. Although Dr. Atlas avoids using names in several cases, a number of President’s Trump staff come across as young, inexperienced, perhaps well-meaning but clearly out of their depth.
Dr. Atlas and his colleagues had some success influencing the actual policies in Florida, although according to the book Governor DeSantis seems to have largely made up his own mind from reading the direct scientific literature and studying the actual data, using experts like Dr. Atlas, Harvard epidemiologist Martin Kulldorf, Oxford epidemiologist Sunetra Gupta, and his Stanford colleague Jay Battacharya as a sounding board to check his understanding. Although Dr. Atlas describes a few successes at the federal level, he had no real success at the national, federal level or with most states and state governors. While he is highly critical of the medical advisers Fauci/Birx/Redfield and even President Trump who hired him, he performs little analysis of his own failings — a trait most of us share.
Missing References and Data
The book does not have end notes or footnotes with primary references, despite Dr. Atlas’s background as an academic scholar and the highly technical nature of the issues. He presumably has a list of key references that he used as policy adviser to the White House that could have easily been incorporated into the book. He makes the point repeatedly during the book that he spent every day reviewing the latest research papers and COVID data, whereas the Fauci/Birx/Redfield “troika” seemingly did not.
The lack of primary references (or any references at all) is a serious drawback because Google and other online searches, even with the less censored DuckDuckGo search engine, often turn up hysterical mainstream news articles and “Fact Checks” rather than the primary references. Readers who have followed the technical literature and non-mainstream arguments closely will not find anything new technically in the book, but others who rely on the mainstream media likely will find contradicting claims and “information” using a search engine, even DuckDuckGo.
Dr. Atlas’s Wikipedia page (Jan 26, 2022), for example, is highly negative:

Wikipedia entry for Scott Atlas (Jan. 26, 2022)
The ineffectiveness of masks is the only technical issue out of many in the book where Atlas presents actual data in plots on pages 287-294 showing no effect from mask mandates on daily news cases in many different countries and US states (yes, theoretically mask mandates could fail although masks work and Atlas does not address this counter-argument). He does not provide primary references even for these plots.
There was and is a substantial scientific literature showing masks, especially the cloth masks, are largely or completely ineffective or even harmful. Atlas provides no references to this literature. Given the remarkable contradiction on masks and other topics between most mainstream sources such as Wikipedia and highly visible statements on cable and broadcast “news” shows by ostensible experts such as Dr. Fauci and Atlas’s claims in the book, Atlas clearly should provide primary references for incredulous readers.
Although there is much discussion of masks in the book including assertions that SARS-COV-2 is airborne, that is it floats in the air like tiny smoke or dust particles and does not drop to surfaces under gravity as larger droplets of saliva would, Dr. Atlas fails to provide references or adequately describe this key technical issue.
In particular, observers have suspected that plagues, especially respiratory illnesses, were airborne since ancient times. Mask wearing has frequently failed during historical epidemics such as the 1918 influenza epidemic. “Public health” authorities have either ignored the historical failure or rationalized it away.
In the 1950’s and 1960’s a team of researchers led by Richard Riley at Johns Hopkins University conducted an extensive series of experiments at a VA hospital showing that tuberculosis, a bacteria which is much larger and heavier than the influenza virus or the coronaviruses, is airborne. They did this by connecting tuberculosis (TB) wards at the hospital to rooms with guinea pigs via air ducts, otherwise isolating the guinea pigs from possible sources of infection, and placing ultraviolet (UV) sterilizing lights in one duct to one room of guinea pigs. The guinea pigs in the room with the UV lights in the connecting duct did not contract TB whereas the guinea pigs in the other room with no sterilizing UV light in the connecting duct did contract TB.
Although it is now “generally accepted” that TB is airborne, “public health” authorities have continued to claim all other respiratory illnesses are transmitted by large saliva droplets that fall to the ground and other surfaces quickly under gravity. This claim was used to justify the “social distancing,” mask wearing, lockdowns, and other policies that have clearly failed to contain COVID and yet continue.
Magically, perhaps as citizens began to realize that heavy droplet transmission would imply rapid efficient spread through groceries at giant stores such as Safeway, Walmart, and Target that were allowed stay open while smaller competitors serving small local regions were closed, the US CDC flipped and claimed “fomites,” meaning those saliva droplets landing on grocery products, store shelves, etc. did not spread the disease — “just kidding.” More precisely they began to claim the surface transmission was so minor that cleaning with various chemicals was no longer recommended.
Remarkably, the “public health” authorities appear to have never replicated the Johns Hopkins TB study or performed similar studies for influenza or coronaviruses despite multi-billion dollar CDC and NIH budgets and continual publicly stated concern about repeats of the 1918 “flu” pandemic.
The practical consequences of airborne transmission are profound. Masks are not expected to work as the tiny viral particles, about 1/500th the width of a human hair, will flow with the air through even microscopic holes in masks, and with the air around the masks. Confining large numbers of people to apartment complexes with interior hallways or shared ventilation is likely to rapidly spread any respiratory disease. People confined in the same house are all likely to be exposed to the virus. Herding everyone into a few small enclosed giant “Big Box” stores such as Walmart or Safeway is likely to provide an efficient route for rapid spread of the disease. Social distancing is likely to be mostly ineffective especially indoors as the viral particles diffuse through any enclosed space.
Curiously, A Plague Upon Our House, despite correctly pointing out the failure of the masks, does not delve into the key issue of airborne transmission and its implications.

Trump: Indecisive or Disingenuous?
Although most of Atlas’s criticism is directed at the seemingly incompetent “troika” of Anthony Fauci, Deborah Birx, and Robert Redfield, he is also highly critical of Trump who in fact supported the policies promoted by the troika, despite occasional tweets seemingly to the contrary. Atlas describes Trump as friendly to him and always agreeing with Atlas in private conversations. Atlas is mystified by Trump’s failure to act on his stated beliefs as shared with Atlas, blaming this both on the troika and various Trump advisers rather than Trump personally. Atlas either failed to consider Trump might be pretending to agree with him or chose not to discuss that possibility in his book.
President Trump is a highly successful businessman at one point deeply involved in the rough and tumble casino industry — even taking over Resorts International, a notorious company with a scandalous past. He has a long history of close personal and business “relationships” with murky, rather iffy characters such as the late attorney Roy Cohn, the late singer Michael Jackson, and the late “hedge fund billionaire” without an actual hedge fund Jeffrey Epstein amongst others. That Trump might be something less than straightforward with Atlas or others does not seem improbable.
The actual voting base of Trump is not Pfizer or Bill Gates/Moderna or other giant companies like Walmart or Safeway, it is small business owners, farmers, and large numbers of working class Americans, many employed by small businesses. Atlas briefly notes that Trump’s FDA commissioner Scott Gottlieb took a lucrative position as a member of the board of directors of Pfizer. Atlas does say he disagreed with Gottlieb strongly, but claims he did not attribute Gottlieb’s positions to a conflict of interest with Pfizer. Preteritio?
President Trump had expressed some vaccine skepticism during the 2016 campaign, even suggesting that vaccines might play a causal role in the dramatic increase in autism in the United States over the last three decades. He apparently did reach out to Democrat vaccine skeptic Robert F. Kennedy Jr to pursue a detailed audit of the seemingly confidential public health databases used by CDC and other agencies to clarify the situation.
Robert F. Kennedy Jr. attributes the sudden reversal on this project during the transition period to a large contribution to the Trump inauguration fund by Pfizer. According to Federal Election Commission (FEC) filings, Pfizer donated $1 million dollars to the 58th Presidential Inaugural Committee on December 22, 2016 (see page 163 of the linked 510 page FEC document).
Pfizer has a long history of criminal activities, including an international conspiracy in the 1990s with Archer Daniels Midland and several other companies to fix the price of citric acid (a key ingredient of Coca-Cola amongst other products), lysine, and possibly other food additives.
The lockdown policies have been disastrous for these more ordinary Americans while enriching Amazon and other Big Tech companies, giant retailers such as Walmart and Safeway, and indirectly the vaccine makers like Pfizer. Unrest and opposition to the policies surfaced quickly among President Trump’s base, many of whom, contrary to the Democrat picture of mesmerized cultists, are wary of the flamboyantly sleazy casino magnate turned champion of the common man.
It is not uncommon for politicians to pay lip service to the opinions and policies preferred by their voters while in fact enacting the policies preferred by their campaign contributors and business partners.
Lack of Criticism of Operation Warp Speed
A major weakness of the book is Dr. Atlas’s unreserved enthusiasm and endorsement of Operation Warp Speed and the experimental mRNA based vaccines. Although he does not devote much space to this, it is crystal clear in reading the book. He writes approvingly about the policy to exempt the vaccine makers such as Pfizer and Moderna from liability should the vaccines prove harmful.
Dr. Atlas expresses no concern that vaccines based on the SARS-COV-2 spike protein which bonds to the ACE-2 (angiotensin converting enzyme) receptor and appears to severely disrupt the cardiovascular system, causing the often lethal blood clots reported in some COVID patients, might produce similar cardiovascular problems in vaccinated persons, although he does oppose vaccine mandates and the unscientific ignoring of natural immunity in statements by the “public health” authorities, the troika until recently, and others.
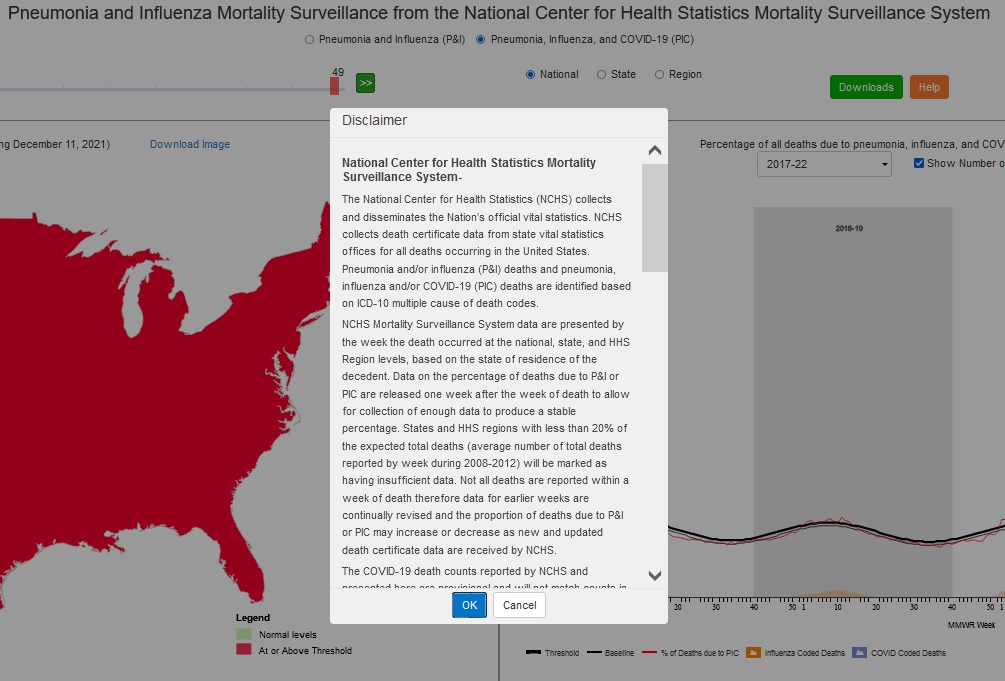
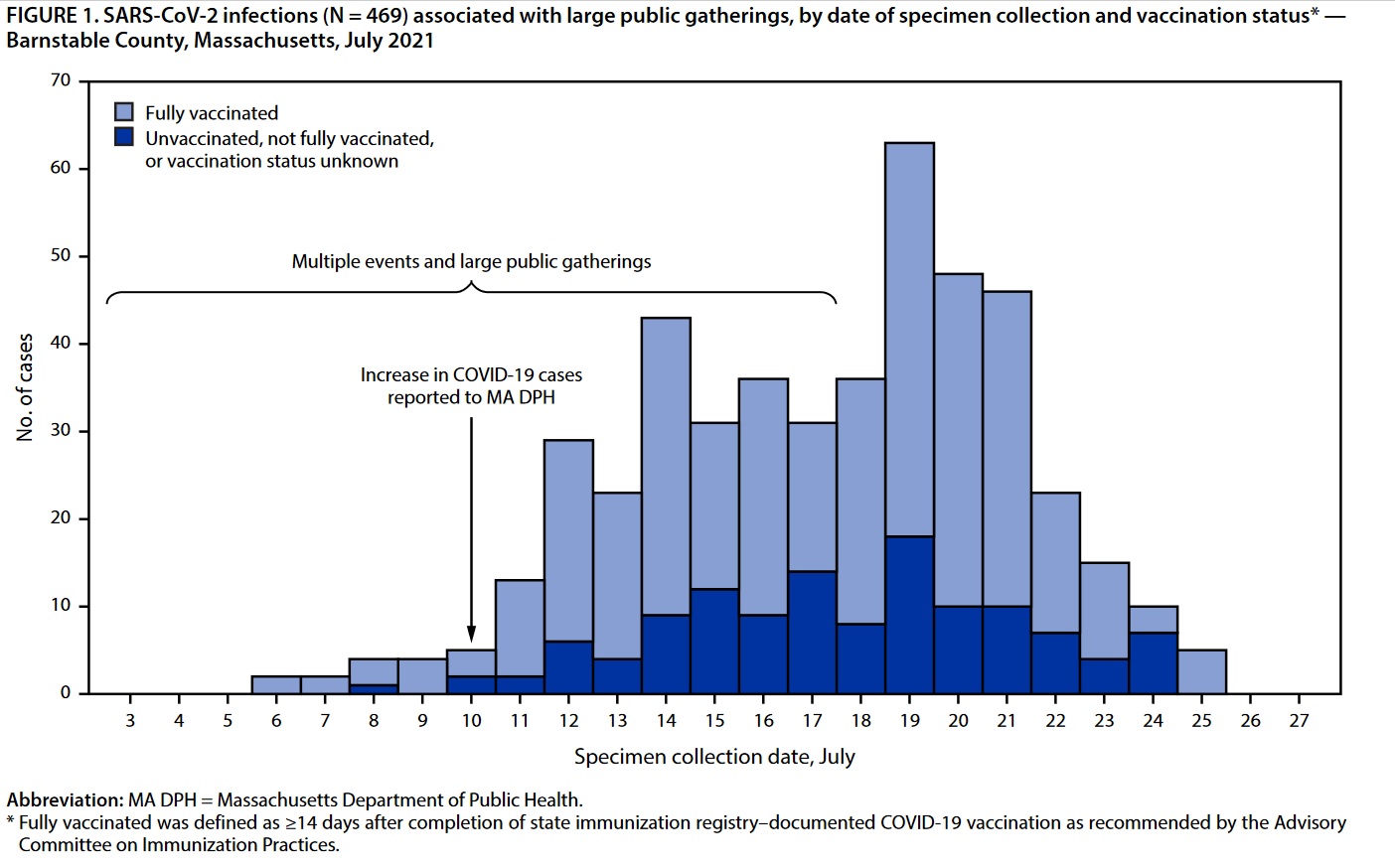
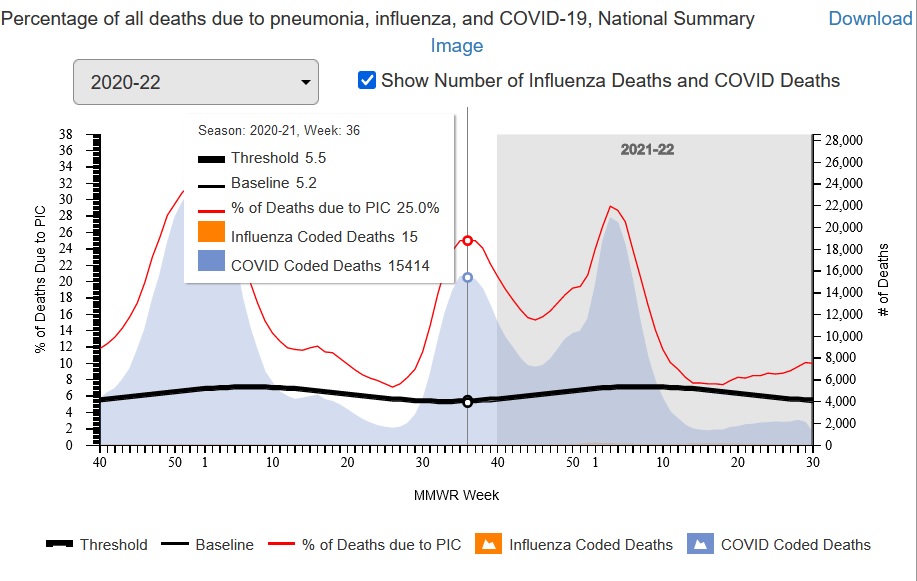
According to the book, Dr. Atlas wrote or completed writing the book in August 2021, arguably just before or as the delta wave was starting to smash through the vaccines, hospitalizing and killing large numbers of Americans if you believe the CDC’s Fluview web site and underlying data as reported.
Dr. Atlas expresses no concern about the short circuiting of numerous safety precautions that usually take years to approve a vaccine. Operation Warp Speed met its hyper-aggressive schedule as Atlas proudly claims only by disregarding established safety measures which he does not mention.
In some contexts, usually when making excuses for obvious failures or huge cost and schedule overruns which are common in R&D, scientists such as Dr. Atlas often claim an 80 to 90 percent failure rate for scientific research. For every Manhattan Project that succeeded there are dozens of tokamak fusion power programs, wars on cancer, and so on that have failed. Yet, Dr. Atlas expresses no concerns or fallback plans for the likely failure of Operation Warp Speed if the 80 to 90 percent failure rate is true.
Lack of Self Criticism
Although Dr. Atlas is highly critical of the troika and even President Trump, he does not take himself to task even though he clearly failed to achieve the policies he recommended, citing only a few small successes. This is something of relevance to all of us who seek better policies and to end the irrational hysteria about the COVID pandemic.
Dr. Atlas does claim he was naive about the political process and how politicized the COVID response was. He also is appalled by the censorship, propaganda, and extensive lying or at least false statements by the mainstream media, both “legacy” operations such as the New York Times and social media giants such as YouTube (owned by Google/Alphabet). Other than being outraged, he makes little effort in the book to analyze how and why this is happening and how to successfully combat it.
One may wonder about these claims of naivete given that Dr. Atlas is a fellow at the controversial, mostly conservative Hoover Institution at Stanford University where he has been a health policy analyst for years. The Hoover Institution as a whole is no stranger to bitter partisan political battles.
In any case, Dr. Atlas makes no attempt to understand the crazed “no lie is too big,” “no number of COVID deaths is too many” to GET TRUMP AT ANY COST mentality of the mass media and many others. Indeed this behavior is puzzling and alarming, leading naturally both to psychological explanations such as the “mass formation” theory proposed by Professor Mattias Desmet and grand “conspiracy theories” of varying degrees of seeming plausibility such as those about Klaus Schwab, the World Economic Forum, and the “Great Reset.”
The Collective Fight or Flight Response
Certainly, whether by design (conspiracy) or accident or a mixture of both, we are experiencing a collective fight or flight response on a nearly global scale, a natural response in ancient times when your tribe is attacked by another tribe, in which masks and vaccination are shibboleths to identify friend and foe, like the phrase “lollapalooza” reputedly used by American soldiers in the Pacific during World War II to separate native English speaking US soldiers from Japanese soldiers especially at night.
The collective fight or flight response is the same response that caused massacres of alleged witches, vagabonds, Jews, and others accused of poisoning wells during the Black Death. The fight or flight response is instinctual, overriding higher cognitive functions. High intelligence and formal education does not prevent it or increase one’s ability to shut it off when it is unwarranted — an overreaction for example. It is hard coded into all or nearly all human beings: rich and poor, ignorant and highly educated, dumb and super-smart.
Social conformity, hostility to dissent, censorship, and propaganda all increase markedly during historical episodes of the collective fight or flight response such as during both World Wars. Because of the demonic imagery associated with the Nazis and the Holocaust, it is easier to see the irrationality of the response in World War I than World War II. It is however an irrational, instinctual response rooted in a direct physical attack by a rival tribe in ancient times, not adapted to even modern wars let alone pandemics.
Trump as the American Hitler
Regardless of the motives of any elite conspiracy, Donald Trump’s surprise victory in 2016 caused a collective fight or flight response based on a deep seated belief in and fear of an “American Hitler,” among many Americans, disproportionately liberal Democrats, an insane, evil demagogue who would capture the votes of hillbillies and other stigmatized mostly poor rural whites and lead the US and the World to destruction.
This frightening archetype is common in US popular culture and serious scholarship, dating back at least to the fears of and historical reactions to William Jennings Bryan and most importantly the crusade against Louisiana Senator Huey Long culminating in Long’s assassination in September of 1935, painting Long as the US equivalent of Hitler.
If you believe Trump is the American Hitler, a secular liberal progressive equivalent of the Antichrist figure of the Book of Revelations, then anything is justified to stop him: lying, cheating, stealing, even advocating policies that will in fact increase deaths during a pandemic to undermine him, particularly given the spectre of global thermonuclear war even though the “American Hitler,” Trump, shows a marked antipathy to global thermonuclear war.
Completely irrational behavior such as trying to stop efforts to make deals with Russia and North Korea becomes justifiable if Trump is the American Hitler. Even loopy ideas like provoking a conflict with nuclear armed super-power Russia over Ukraine (currently in the news) to rally the public and prevent Trump or a Trump successor from returning in the mid-term elections may seem reasonable to otherwise intelligent people. Keep in mind if the Trump Republicans were to gain a super-majority in both houses in the 2022 election, they could in principle invalidate the contested 2020 election and restore Trump in 2022 instead of 2024.
Regardless of how unjustified and perhaps unhinged such beliefs about Trump, potential Trump replacements such as Governor De Santis or Senator Rand Paul, or Trump voters actually are, Dr. Atlas, Trump himself, and others have failed to allay them. Once a group of people or a single person is in the instinctual fight or flight response, reason usually fails until they calm down. It is incumbent upon Dr. Atlas to assess why he failed and how to succeed. This is a major weakness of the book.
Conclusion
A Plague Upon Our House paints an alarming portrait of the US government, President Trump and especially the “troika” of Anthony Fauci, Deborah Birx, and Robert Redfield and their many allies — something of continuing concern given Fauci’s current role in the Biden administration. It is filled with anecdotes suggesting Fauci is either incompetent or something worse.
The book would be stronger and more helpful in the continuing crisis if Dr. Atlas carefully evaluated the reasons for his failure to stop the disastrous policies, inability to reach the public and allay the concerns of frightened “never Trumpers,” and how to succeed now in the continuing crisis.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).