John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Short video discussing results of analyzing President Biden’s declining approval ratings and the possible effect of the COVID pandemic and Ukraine crises on the approval ratings.
A detailed longer explanation of the analysis discussed can be found in the previous video “How to Analyze Simple Data Using Python” available on all of our video channels.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Video on how to analyze simple data using the Python programming language using President Biden’s approval ratings as an example.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Video on how to perform a simple analysis of simple data in LibreOffice Calc, a free open-source “clone” of Microsoft Excel. Demonstrates how to use the Trend Line feature in LibreOffice Calc Charts. Discusses how to use the R Squared goodness of fit statistic to evaluate the analysis.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Russia invaded Ukraine on February 24, 2022, temporarily moving the COVID-19 pandemic, pandemic response, and the huge number of COVID cases and deaths worldwide attributed to the Omicron variant of SARS-COV-2 despite high levels of vaccinations and masking. So far however, President Biden does not appear to have gotten a boost from the rally around the flag/leader effect that, for example, boosted President George W. Bush’s approval ratings dramatically after the September 11, 2001 mass murder incidents, usually described as attacks on the United States. To be sure, so far there has not been a “New Pearl Harbor” such as 9/11 or a cyberattack or other direct attack on the United States blamed on Russia.
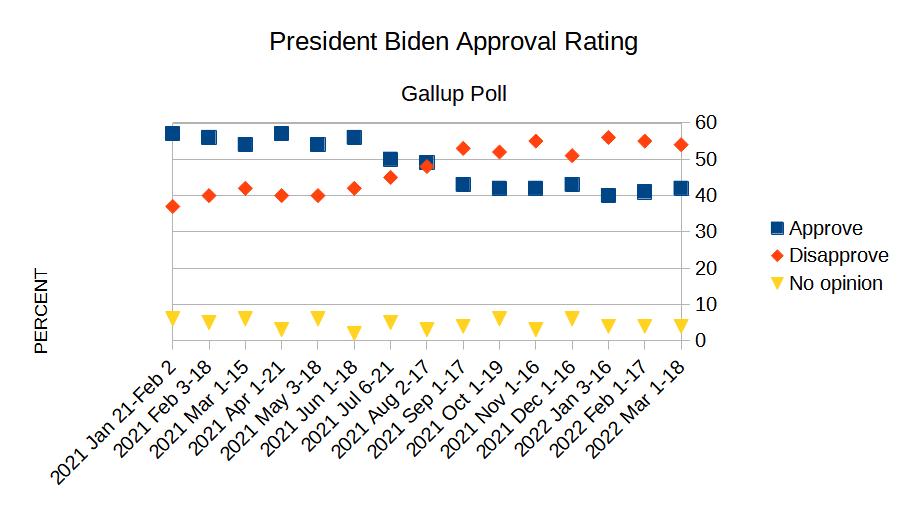
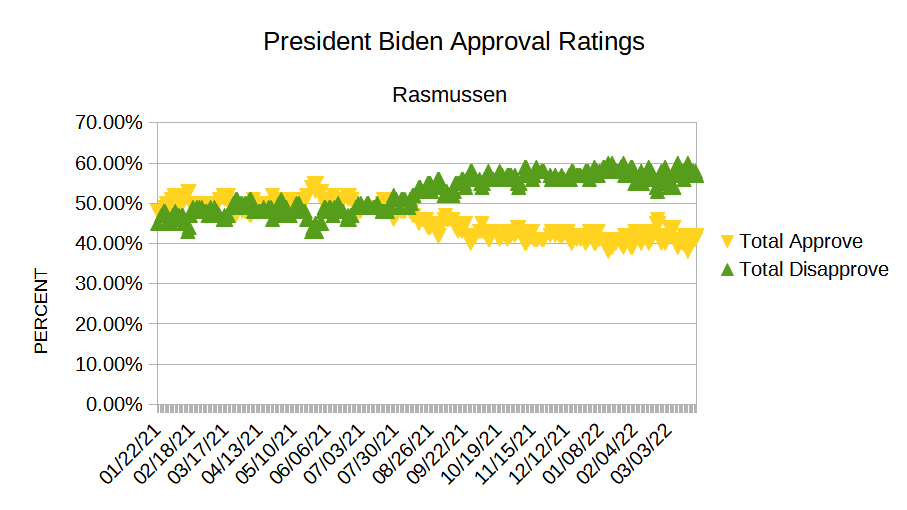
Biden’s approval rating continues to drop (March 27, 2022)
Polling data from Gallup, Rasmussen, and a broad sampling of popular polls all show no clear boost given the few probably few percent error rate of the polls, even a small one, from the Ukraine-Russia crisis so far:
All of the polls show a marked drop in Biden’s approval ratings in July-August of 2021. One cannot be certain of the reasons, of course, but this is when it became clear that the COVID vaccines worked poorly at best and did not prevent infection or transmission in the vaccinated, contrary to prominent super-confident statements by Biden and his administration that the vaccines would prevent infection in the vaccinated (something obviously untrue from the Pfizer and Moderna clinical trials reports which reported some infections in vaccinated trial subjects).
The approval rating plots above were made with data copied from the referenced web sites on March 27, 2022 and plotted in LibreOffice Calc spreadsheet, a free open-source spreadsheet program similar to Excel, loosely an Excel “clone” although there are some differences.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The omicron variant of the SARS-COV-2 virus, widespread testing including the newly available (in US) antigen tests, or some combination of these factors has resulted in a huge number of both cases and deaths attributed to SARS-COV-2 despite widespread vaccination. Cases and deaths have soared in groups and regions such as Israel and the UK reporting very high vaccination rates, making attributing the cases to the “unvaccinated” implausible.
This has put public health authorities such as the US Centers for Disease Control and Prevention (CDC), WHO, and other agencies around the world in a bind. At best, the soaring cases and deaths reflect either extensive failure of the current vaccines or high false positive rates in the various tests resulting in other respiratory disease cases and other deaths being misidentified as COVID-19.
For the sake of argument, accept that the vaccines are quite safe despite the alarming VAERS data in the United States and that, as widely claimed, the vaccines do confer some reduction in death and severity of illness for a brief few month duration, nonetheless the huge number of cases and deaths throughout the world suggests that the vaccines are largely ineffective in real-world conditions. This may be due to omicron mutating around the vaccine induced immunity based on earlier variants of SARS-COV-2, the frequent waning of the immunity conferred by inactivated vaccines, or even other causes not identified.
This failure of course is an embarrassing debacle at best for public health authorities and agencies, political leaders, and various billionaire philanthropists, particularly because the costly and disruptive lockdowns were justified to protect the vulnerable until a life-saving vaccine would be available – despite the well known high failure rate of research and development, often estimated at 80-90 percent.
However, if current omicron cases and deaths reflect high false positive rates, the past case and death counts since March of 2020, often described by public health authorities or mainstream news reports citing unnamed public health authorities when reported as both “undercounts” and highly accurate are even more suspect than recent numbers. In the United States, the CDC has previously explained the lack of real time data reporting and other flaws in the COVID-19 case and death data, causing officials to rely on data from the UK and Israel, as caused by antiquated IT systems, lack of funding in previous budgets, alleged cuts by the Trump administration, and similar excuses.
Many of the early tests were produced in haste, rushed out under experimental use authorizations (EUA), including an embarrassing failure by CDC early in the pandemic to produce a usable PCR test (URL: https://arstechnica.com/science/2020/04/cdcs-failed-coronavirus-tests-were-tainted-with-coronavirus-feds-confirm/ ). Tests, testing methods and technologies should certainly have improved in the last two years of the pandemic; if not, why not? Especially given the trillions of dollars spent on the pandemic response.
Some mainstream reporting on problems with the US CDC’s data and data handling.
The current crisis in the Ukraine has undoubtedly distracted much of the public from the omicron bind. Nonetheless the soaring cases and deaths attributed to the omicron and post-omicron variants of SARS-COV-2 appears to reveal gross contradictions in the claims by public health authorities about the COVID pandemic. While it is usually possible in practice to find some convoluted, acrobatic explanation for obviously contradictory data and/or logic, such explanations are rarely true.
Improper Scientific Practice
The public health authorities are portraying the flip flops and contradictions in their assertions about COVID as brilliant scientific discoveries — new science or the science has changed — although that excuse is wearing thin. This is not how proper science functions — even major breakthroughs. It proceeds from tentative statements and numbers with large error bars and/or broad confidence intervals to smaller and smaller errors as more data, better measurements, and better models are developed.
Error bars are graphical representations of the variability of data and used on graphs to indicate the error or uncertainty in a reported measurement. They give a general idea of how precise a measurement is, or conversely, how far from the reported value the true (error free) value might be. Error bars often represent one standard deviation of uncertainty, one standard error, or a particular confidence interval (e.g., a 95% interval). These quantities are not the same and so the measure selected should be stated explicitly in the graph or supporting text. Error Bars, Wikipedia, March 25, 2022
Science rarely jumps from super-confident statements such as “masks don’t work” to grossly contradictory super-confident statements such as CDC Director Robert Redfield’s ludicrous “masks will stop the pandemic in 8-12 weeks” statements in the summer of 2020. (LINK: https://people.com/health/americans-wore-masks-drive-this-epidemic-to-the-ground-says-cdc-director/ ) That sort of a jump or contradiction usually indicates bad science — gross underestimation of the errors before or after the jump (or both). In most cases, the scientific discovery is reflected in a sharp discontinuous drop in the error bars due to a better theoretical and/or mathematical model or better measurements or both.
For example, Johannes Kepler’s discovery of the elliptical orbits of the planets combined with superior measurements with the new telescopes in the 17th century resulted in a dramatic drop in the error bars on predictions of planetary motions from about a one percent (1%) error with the Ptolemaic system to a tiny fraction of one percent. It did not result in a gross reversal of centuries of astronomical observations and predictions. Ptolemy and his successors knew their model was imperfect and said so. Mars did not suddenly stop backing up for two months every two years in 1605 when Kepler realized what was going on. The empirical phenomenon did not somehow reverse overnight, rather our understanding leaped forward and the accuracy of the predictions went up dramatically.
(ABOVE) The red error bars and the dark blue data points show the ideal proper scientific practice in which the reported red error bars include the actual value largely determined in the 2015-2016 period in the hypothetical example shown when the science jumps forward. The green error bars and light cyan data points show improper scientific practice in which the scientists are over-confident both before and after the “breakthrough.”
It is common for over-confident scientists to explain the contradiction by referring to the uncertainty of science as if the poorly educated audience or critic is unaware of uncertainty and as if the scientists properly reported the large pre-2015 red error bars previously whereas they actually reported the incorrect small green error bars. This switch is the scientific uncertainty excuse.
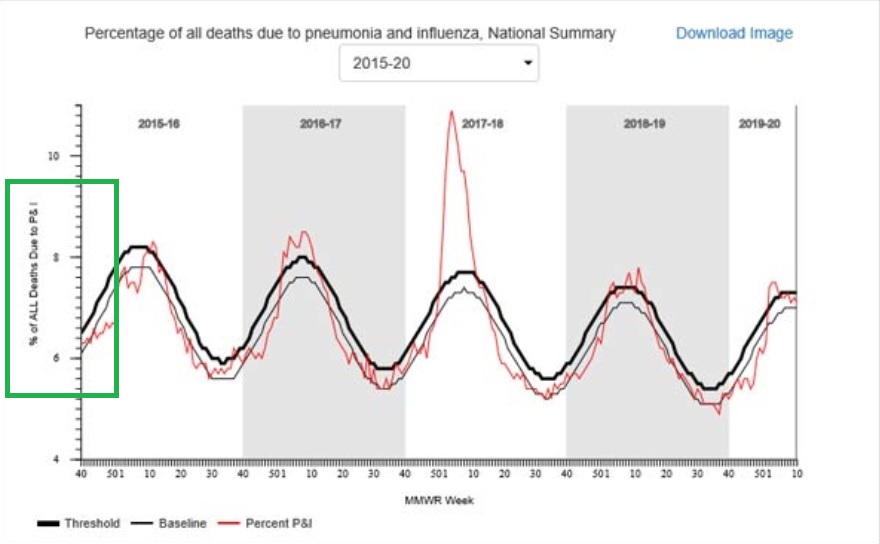
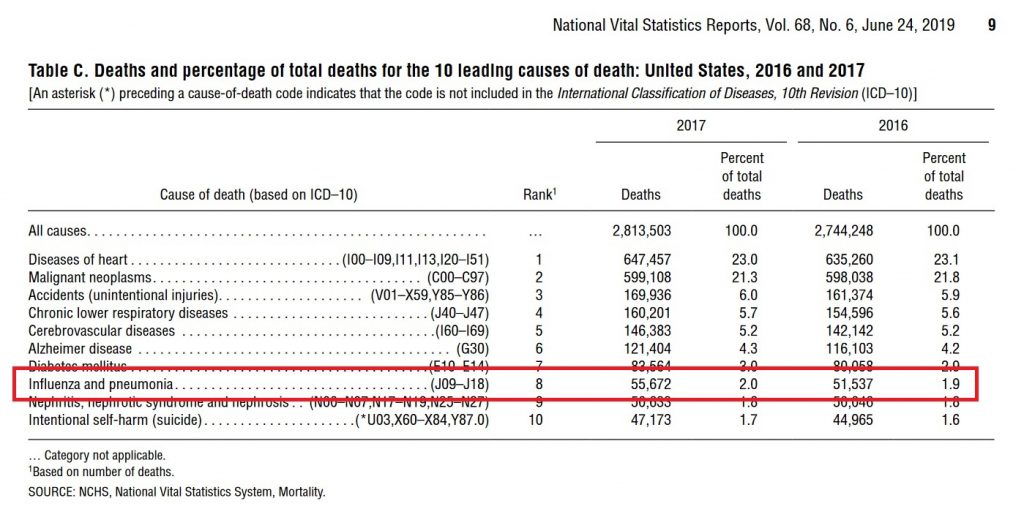
Indeed there is a frequent improper failure to report statistical and systematic errors throughout the public health “science” both as presented to the lay public, on news shows, and in CDC and other web sites and publications. One of the most striking examples is a large difference in the number of deaths attributed to “pneumonia and influenza” on the US CDC FluView website (~188,000 per year) and the US CDC leading causes of death report (~55,000 per year). These grossly contradictory numbers have been reported for years with no statistical or systematic errors, nor clear explanation for the difference. The discrepancy between the FluView website and the leading causes of death report predates the COVID-19 pandemic by several years. This gross discrepancy is likely extremely relevant to the question whether a death is “with COVID” or “from COVID” or some intermediate case.
The CDC FluView website shows that 6-10 percent of all deaths, varying seasonally, are due to (the precise language on the graphic) pneumonia and influenza (P&I) according to the vertical axis label on the FluView Pneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list, as mentioned, ~188,000 deaths per year attributed to pneumonia and influenza.
The CDC FluView graphic and underlying data files list no statistical or systematic errors. The counts of deaths in the data files give the numbers to the last significant digit, implying an error of less than one count, one death, based on common scientific and engineering practice.
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see Figure 3) attributes only 2 percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers seems to be due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not, however, clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some or even many cases. Despite this, none of these official numbers, either in the leading causes of death report or the FluView website, are reported with error bars or error estimates, as is the common scientific and engineering practice when numbers are uncertain. The leading causes of death report for 2017 reports exactly 55,672 deaths from “influenza and pneumonia” in 2017 with no errors– as shown in Figure 2.
It is impossible to perform an accurate cost benefit analysis of any policy without honest reporting of the uncertainties/error bars. The overconfident statements will have serious real world consequences in human lives unless they prove correct through luck.
Generally statements with — in fact — large error bars should not override personal judgment (e.g. mandates) especially in life and death situations. The government may be justified in preventing parents from treating an illness with a fatal dose of cyanide, where the lethality of the “treatment” is certain. The government is certainly not justified in compelling parents to treat an illness with an experimental treatment with large uncertainties and unknowns even if that treatment might save the child’s life.
Scientists have an ethical obligation to honestly compute and report both statistical and systematic errors; this is common scientific and engineering practice taught by accredited universities and colleges throughout the world.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Video on airborne spread of COVID-19 and other respiratory diseases such as tuberculosis and influenza, discussing implications for lockdowns, masks, and other measures. About twenty-five (25) minutes.
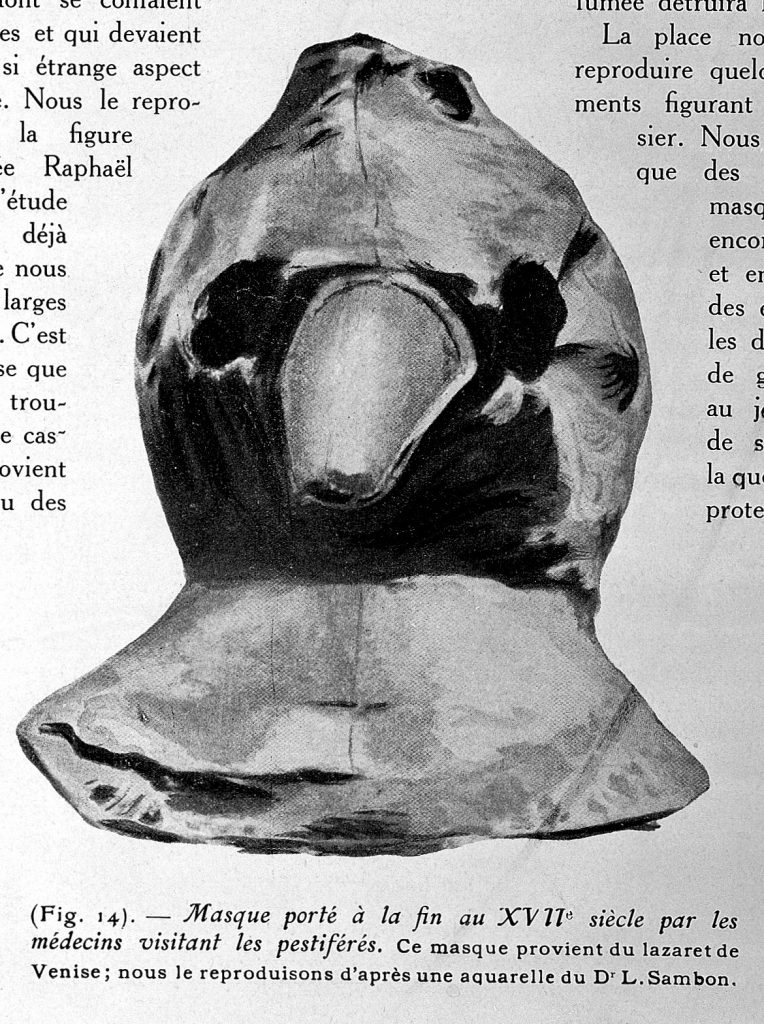
L0025227 Mask used by a plague doctor
Credit: Wellcome Library, London. Wellcome Images
images@wellcome.ac.uk
http://wellcomeimages.org
Mask used by a plague doctor: Masque porte a la fin au XVIIe siecle par les medecins visitant les pestiferes. Ce masque provient du lazaret de Venise; nous le reproduisons d’apres une aquarelle du Dr. L. Sambon.
Photograph
Aesculape
Published: 1932
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0 http://creativecommons.org/licenses/by/4.0/
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Unmasked: The Global Failure of COVID Mask Mandates
By Ian Miller
Post Hill Press, New York, 2022
Unmasked is an easy-to-read graph-filled book that makes a very strong case that masks, also known as face coverings, have little or no effect on infection, transmission, hospitalization or death due to COVID-19 and may even be somewhat harmful. Although the book does not quantify what “little” might mean, one of several weaknesses of the book, it likely means at most a few percent reduction. After nearly two years of COVID-19 and masking, this should be pretty obvious and non-controversial, but it remains a highly contentious topic with the United States CDC continuing to produce and promote dubious mask studies claiming or implying high levels of mask effectiveness. Conservative commentator Dan Bongino was recently deplatformed by YouTube (Google/Alphabet) ostensibly for asserting that masks don’t work (or cloth masks don’t work according to some accounts).
The book discusses how the “settled science” before the end of March 2020 was that masks had little or no benefit as shown by many prior studies. Masks had in fact clearly failed during the infamous 1918 influenza epidemic. This was reflected in now infamous public statements by Anthony Fauci, US Surgeon General Jerome Adams, and other “experts.” The “settled science” reversed one-hundred and eighty degrees at the beginning of April 2020 with Fauci subsequently claiming his original statements were a lie, now usually described as a “noble lie” to save N95 masks for health care workers.
The book devotes several short readable chapters to masks and the flu (meaning the influenza virus), the CDC pro-mask studies, the US states California and Florida arguably representing the two extremes on mask policy, Sweden which largely eschewed masks, and international comparisons.
The climax of the book is a long, dense chapter going alphabetically through all US states and Washington DC, with a graph of daily new cases per million population for each jurisdiction during the pandemic, graphs annotated with start and stop dates of mask mandates, a few measurements of mask compliance rates, and notable news articles either extolling the mask policy in the state shortly before cases skyrocketed or predicting disaster following removal of a mask mandate, followed by continuing sharp drops in the daily new cases.
The chapter closes with a bar chart showing age adjusted death rates for all US states (no Washington D.C.) sourced in tiny almost unreadable type to the US CDC, from the highest age adjusted death rate (New Jersey with about 140 COVID deaths per one-hundred thousand residents) to the lowest (Vermont with about 15 deaths per one-hundred thousand). States without mask mandates or minimal mask mandates are highlighted, spanning nearly the entire range with South Dakota as 3rd worst state just behind Number 2 New York and Alaska at 46. High profile Florida falls at forty in the graph with about 55 deaths per one-hundred thousand. This is for the twelve month period thru the fourth quarter (Q4) of 2020.
The plots and other data in the book make a strong case that masks at best only have a small positive effect that must nearly always be swamped out by other factors which the book largely does not discuss.
Several Weaknesses
The book appears to be largely aimed at conservative, libertarian, pro-Trump or anti-(anti-Trump) audiences. By anti-(anti-Trump) is meant the many people who fall somewhere between unenthused about Trump to quite concerned but view the “get Trump at any cost” reaction to Trump as a dangerous, irrational overreaction. The anti-(anti-Trumpers) span the conventional political spectrum and arguably include such prominent figures as Glenn Greenwald, former Rolling Stone writer Matt Taibbi, and podcaster Joe Rogan. The book features advanced praise quotes from libertarian author Tom Woods, conservative commentator Ann Coulter, and similar figures on its first page.
While the book does have references, these are all or nearly all popular news articles and not scholarly peer reviewed scientific journal articles of which their are many, pre-prints, or similar non-peer reviewed content (e.g. “working papers”). The numerous plots do have a reference in tiny print at the bottom, almost unreadable. These references are often secondary sources such as Worldometer or the New York Times COVID dashboards etc. This is better than Scot Atlas’s A Plague Upon Our House, also from Post Hill Press, which has no references despite the author emphasizing the importance of scientific references in critiquing Anthony Fauci and others. However, the book should have scholarly references and links to primary data sources such as the CDC web site.
The plots are quite small. The printed book is about 5 1/2 inches wide by 8 1/4 inches high with nearly all plots about 4 inches wide by 2 1/2 inches high with small to very tiny type, undoubtedly hard for many readers. It probably would have been better to devote an entire page to each plot for clarity.
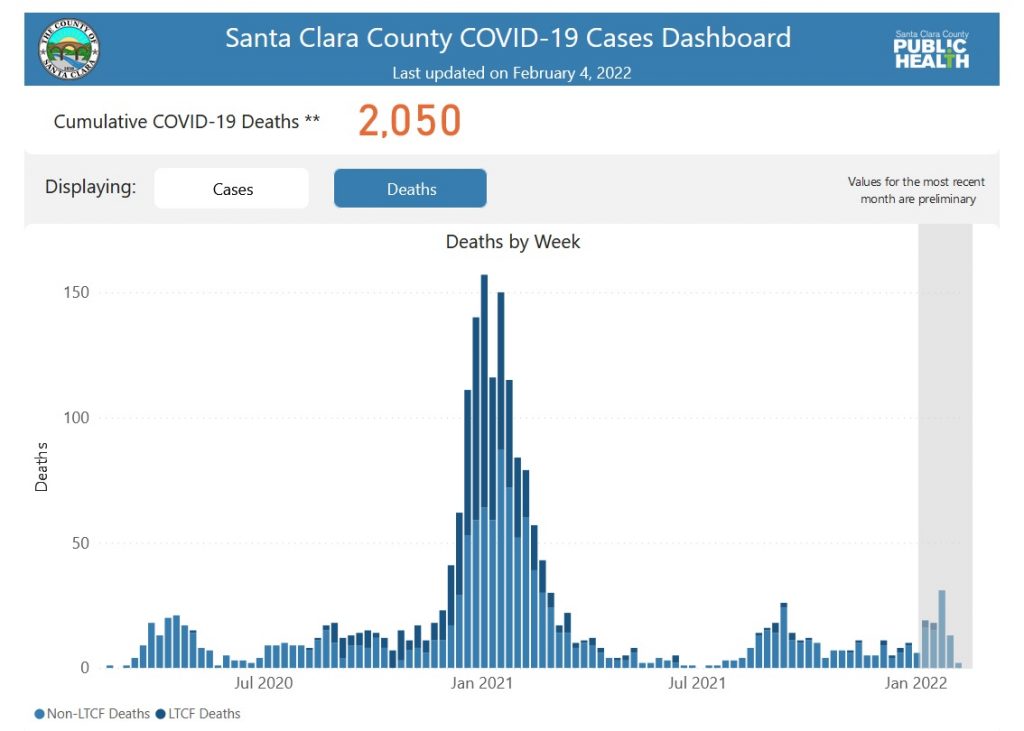
The book should devote more space to the issue of mask compliance. Quite clearly the mask mandates failed, but the fallback argument is that the people, especially knuckle dragging Trump supporters, failed to follow the mask mandates. The book does cite several studies of mask compliance — actual mask wearing — contradicting this explanation. Living in the San Francisco Bay Area, I am personally sure mask compliance was high in the SF Bay Area and likely other urban centers such as LA and San Diego. But even in California, the failure could be blamed on rural Californians. In fact, COVID-19 deaths soared in urban Santa Clara County during the winter of 2020-2021 despite the heavy use of masks.
COVID-19 Deaths in Santa Clara County (SF Bay Area/Silicon Valley)
The weakest part of the book is the fourth chapter on the CDC’s handful of highly promoted studies claiming or implying dramatic benefits from mask wearing. These are of course highly contradicted by the mountain of data in the final chapter as well as other chapters. Nonetheless some of the arguments seemed rather weak relying on typical assertions made during scientific and political controversies. Accusations of “poor scientific or statistical methodology” are common and need to be specifically backed up.
The book would be stronger with a chapter on why masks might fail. The likely explanation is that there is practically significant aerosol transmission of COVID-19, meaning the virus floats in the air like fine dust or smoke. The viral particles are tiny, too small to be seen by an optical microscope, about 1/500th the width of a human hair. They can easily flow through the mesh of cloth or surgical masks. The N95 masks claim to stop 95 percent of particles 0.3 microns (300 nm) in diameter. The coronavirus is about 0.14 micron (140 nm) in diameter. The N95 masks probably stop less than 95 percent of such small particles. In theory even one viable viral particle can infect and kill a person.
The book would also benefit from a chapter on the downsides of masks which reduce air intake, trap carbon dioxide, interfere with communication, and have other negative effects. Masks are not advised for persons with asthma and various other respiratory problems. How well can we determine who can safely wear a mask and for how long. OSHA has strict limits on mask use in work settings that would preclude the use of masks to try to control COVID-19.
The book would be stronger by quantifying the bounds on the effectiveness of masks and discussing under what conditions these quantitative bounds apply. This is likely to be a range from negative a few percent (makes things worse) to positive a few percent (weak benefit).
Some articles that review the primary scientific literature in more and better detail than Unmasked are:
All have some weaknesses and suffer from the politicization of the mask issue in various ways, but overall complement the weaknesses of Unmasked.
At this point, with huge numbers of fully vaccinated, mask wearing persons contracting the Omicron variant or at least getting sick and getting test results interpreted as Omicron, it should be clear that masks are largely ineffective, just as was the case during the 1918 influenza epidemic. Rather than beating a dead horse, public discussion and efforts to mitigate the COVID-19 pandemic should focus on more promising options such as UV lighting in ducts and ventilation systems, installation of air purifiers with UV sub-systems to kill viral particles in the air, as well as other possibilities which avoid the enormous social and psychological costs, not to mention physical health risks of prolonged mask wearing.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Pandemia: How Coronavirus Hysteria Took Over Our Government, Rights, and Lives
Alex Berenson
Regnery Publishing, Washington, D.C., 2021
Pandemia is a detailed, somewhat technical history of the COVID pandemic and COVID response mostly in the United States strongly critiquing much of the mainstream news coverage, the lockdown and masking policies, and many claims and policies promoted by the US CDC, Anthony Fauci, and other “public health authorities.” Alex Berenson is a former New York Times investigative reporter who covered many pharmaceutical stories and scandals while working at the Times. I first encountered him through his 2004 book The Number about manipulation and outright fraud in reported quarterly corporate earnings.
The book is written in a breezy, easy to read style with short topical chapters in a roughly chronological order. It has numerous footnotes with a footnote section at the end of the book as well as an index, all to back up his many assertions that differ from most mainstream news coverage, statements by Fauci and other “experts,” and the supposed consensus of scientists. Readers who have been following non-mainstream coverage of the pandemic and pandemic response from sources such as Berenson will not be surprised or find much new. Overall it is a well written, informative book that conveys Berenson’s positions with references to supporting information.
Some Weak Spots
I am not a Conspiracy Theorist
Berenson is adamant that he is not a “conspiracy theorist,” the dread phrase used to shut down any discussion of possible criminal conspiracy or even incompetence by the powerful (such as the “conspiracy theory” that NIH funded “gain of function” research at the Wuhan Institute of Virology produced and then accidentally released SARS-COV-2). Consequently, while he documents baffling failures, claims, and outright contradictory statements by Anthony Fauci, the CDC, and other “public health authorities” such as the dramatic reversal on the effectiveness of masks from “useless” to “highly effective” in April 2020, he stops there and rains scorn on “conspiracy theorists.”
Twitter Warrior
Berenson was eventually banned by Twitter for alleged “COVID misinformation” following what Berenson argues is pressure by the Biden administration and other political figures. He describes many provocative and sometimes offensive tweets which drew a lot of attention to himself, undoubtedly boosting sales of his Unreported Truths booklets on Amazon and now his Pandemia book. He mentions some criticism by his wife Jackie of the aggressive, snarky tone and content of many of his tweets. His substack posts continue to show a similar aggressive, snarky tone today.
Long, Long COVID (Chapter 25)
Berenson is highly skeptical of alleged “Long COVID,” linking it to a range of murky diseases such as chronic fatigue syndrome, fibromyalgia, chronic Lyme disease, and others with arguably similar symptoms which also tend to disproportionately affect women, suggesting a psychological/anxiety cause. He argues that scientists and medical doctors have so far been unable (he says) to find an underlying biological cause or correlate (more on this in a moment) whereas they supposedly found the cause of AIDS (the HIV virus) in only two years. Touting modern high tech molecular biology based science and medicine, he argues it could not be that hard to find a cause if these disease were “real.”
Blaming anxious hysterical women for phantom diseases that disproportionately affect women is not a new phenomenon. Multiple sclerosis (MS) was considered such as disease until a series of autopsies of patients showed lesions (damage) to the nerves. Today MS can be detected with magnetic resonance imaging (MRI) scans which always or frequently show lesions on the nerves in the images.
Both MS and lupus, which disproportionately affect women, continue to be misdiagnosed as psychological problems without an MRI scan or the test for the anti-nuclear antibodies (ANA). About 90 percent of people with lupus (linked article from Lupus Foundation claims 97%) have the unusual anti-nuclear antibodies while only about 5 percent of health individuals have the antibodies. Note that anti-nuclear antibodies are highly correlated with lupus but not perfectly correlated, which raises some questions whether the auto-immune reaction is the true cause of lupus. Alleged auto-immune diseases such as MS, lupus, and rheumatoid arthritis which disproportionately affect women remain mysterious.
MRI scans are unable to image damage to the critical myelin insulating sheath that enclosing nerves. Damage or loss of this sheath which occurs in carpal tunnel syndrome, ulnar and other nerve injuries can be confirmed in many but not all cases with nerve conduction tests. These tests have a several percent failure rate. Damage or loss of the myelin sheath frequently causes extreme levels of pain and in some cases atrophy of the muscles controlled by the nerve.
There are many diseases that have eluded detailed biological analysis. Berenson touts the sequencing of the human DNA as an illustration of the enormous power of modern medical biology without considering about 98% of the human DNA is purported junk DNA whose function is unknown. He extols modern molecular biology research without considering the dismal results of the “War on Cancer” nor the remarkably complex modern theory of cancer with hundreds of oncogenes, allegedly rapidly mutating cancer cells, extensive unpredictable chromosomal changes, and the mysterious anaerobic metabolism seen in many cancer cells.
Could COVID or other disease like Lyme disease occasionally produce some mysterious long lasting, possibly auto-immune syndrome disproportionately in women who disproportionately suffer from alleged auto-immune diseases such as MS, Lupus, and Rheumatoid Arthritis? Quite possibly.
Conclusion
Overall Pandemia is a well written, easy to read book, almost 400 pages of detailed discussion of the COVID pandemic and the lockdowns and other pandemic responses. Berenson makes a strong case that most of the responses have been ineffective at best and even quite harmful in some cases. He avoids speculation about possible conspiracies whether due to genuine skepticism or to avoid the dreaded “conspiracy theorist” label. He stays away from the safety and effectiveness of drugs such as hydroxychloroquine and ivermectin and says little about Vitamin D. He is highly critical of the approval process for the mRNA spike protein based vaccines and the actual real-world safety and effectiveness of the vaccines.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
A Plague Upon Our House: My Fight at the Trump White House to Stop COVID from Destroying America
Scott W. Atlas, M.D.
Post Hill Press, New York, 2021
A Plague Upon Our House is Scott Atlas’s personal account of his four months (“end of July” 2020 — December 1, 2020) as a special adviser to the White House on the COVID-19 pandemic and pandemic response. It also discusses some of his interactions with and advice to Florida state governor Ron De Santis. The book paints an alarming picture of key medical advisers Tony Fauci, Deborah Birx, and Robert Redfield as incompetent, highly political, dishonest career bureaucrats in the worst sense of the words and President Trump as a disengaged, indecisive, publicity obsessed leader quite far from his abrasive, tough, “You’re fired!” public image. Although Dr. Atlas avoids using names in several cases, a number of President’s Trump staff come across as young, inexperienced, perhaps well-meaning but clearly out of their depth.
Dr. Atlas and his colleagues had some success influencing the actual policies in Florida, although according to the book Governor DeSantis seems to have largely made up his own mind from reading the direct scientific literature and studying the actual data, using experts like Dr. Atlas, Harvard epidemiologist Martin Kulldorf, Oxford epidemiologist Sunetra Gupta, and his Stanford colleague Jay Battacharya as a sounding board to check his understanding. Although Dr. Atlas describes a few successes at the federal level, he had no real success at the national, federal level or with most states and state governors. While he is highly critical of the medical advisers Fauci/Birx/Redfield and even President Trump who hired him, he performs little analysis of his own failings — a trait most of us share.
Missing References and Data
The book does not have end notes or footnotes with primary references, despite Dr. Atlas’s background as an academic scholar and the highly technical nature of the issues. He presumably has a list of key references that he used as policy adviser to the White House that could have easily been incorporated into the book. He makes the point repeatedly during the book that he spent every day reviewing the latest research papers and COVID data, whereas the Fauci/Birx/Redfield “troika” seemingly did not.
The lack of primary references (or any references at all) is a serious drawback because Google and other online searches, even with the less censored DuckDuckGo search engine, often turn up hysterical mainstream news articles and “Fact Checks” rather than the primary references. Readers who have followed the technical literature and non-mainstream arguments closely will not find anything new technically in the book, but others who rely on the mainstream media likely will find contradicting claims and “information” using a search engine, even DuckDuckGo.
Dr. Atlas’s Wikipedia page (Jan 26, 2022), for example, is highly negative:
Wikipedia entry for Scott Atlas (Jan. 26, 2022)
The ineffectiveness of masks is the only technical issue out of many in the book where Atlas presents actual data in plots on pages 287-294 showing no effect from mask mandates on daily news cases in many different countries and US states (yes, theoretically mask mandates could fail although masks work and Atlas does not address this counter-argument). He does not provide primary references even for these plots.
There was and is a substantial scientific literature showing masks, especially the cloth masks, are largely or completely ineffective or even harmful. Atlas provides no references to this literature. Given the remarkable contradiction on masks and other topics between most mainstream sources such as Wikipedia and highly visible statements on cable and broadcast “news” shows by ostensible experts such as Dr. Fauci and Atlas’s claims in the book, Atlas clearly should provide primary references for incredulous readers.
Although there is much discussion of masks in the book including assertions that SARS-COV-2 is airborne, that is it floats in the air like tiny smoke or dust particles and does not drop to surfaces under gravity as larger droplets of saliva would, Dr. Atlas fails to provide references or adequately describe this key technical issue.
In particular, observers have suspected that plagues, especially respiratory illnesses, were airborne since ancient times. Mask wearing has frequently failed during historical epidemics such as the 1918 influenza epidemic. “Public health” authorities have either ignored the historical failure or rationalized it away.
In the 1950’s and 1960’s a team of researchers led by Richard Riley at Johns Hopkins University conducted an extensive series of experiments at a VA hospital showing that tuberculosis, a bacteria which is much larger and heavier than the influenza virus or the coronaviruses, is airborne. They did this by connecting tuberculosis (TB) wards at the hospital to rooms with guinea pigs via air ducts, otherwise isolating the guinea pigs from possible sources of infection, and placing ultraviolet (UV) sterilizing lights in one duct to one room of guinea pigs. The guinea pigs in the room with the UV lights in the connecting duct did not contract TB whereas the guinea pigs in the other room with no sterilizing UV light in the connecting duct did contract TB.
Although it is now “generally accepted” that TB is airborne, “public health” authorities have continued to claim all other respiratory illnesses are transmitted by large saliva droplets that fall to the ground and other surfaces quickly under gravity. This claim was used to justify the “social distancing,” mask wearing, lockdowns, and other policies that have clearly failed to contain COVID and yet continue.
Magically, perhaps as citizens began to realize that heavy droplet transmission would imply rapid efficient spread through groceries at giant stores such as Safeway, Walmart, and Target that were allowed stay open while smaller competitors serving small local regions were closed, the US CDC flipped and claimed “fomites,” meaning those saliva droplets landing on grocery products, store shelves, etc. did not spread the disease — “just kidding.” More precisely they began to claim the surface transmission was so minor that cleaning with various chemicals was no longer recommended.
Remarkably, the “public health” authorities appear to have never replicated the Johns Hopkins TB study or performed similar studies for influenza or coronaviruses despite multi-billion dollar CDC and NIH budgets and continual publicly stated concern about repeats of the 1918 “flu” pandemic.
The practical consequences of airborne transmission are profound. Masks are not expected to work as the tiny viral particles, about 1/500th the width of a human hair, will flow with the air through even microscopic holes in masks, and with the air around the masks. Confining large numbers of people to apartment complexes with interior hallways or shared ventilation is likely to rapidly spread any respiratory disease. People confined in the same house are all likely to be exposed to the virus. Herding everyone into a few small enclosed giant “Big Box” stores such as Walmart or Safeway is likely to provide an efficient route for rapid spread of the disease. Social distancing is likely to be mostly ineffective especially indoors as the viral particles diffuse through any enclosed space.
Curiously, A Plague Upon Our House, despite correctly pointing out the failure of the masks, does not delve into the key issue of airborne transmission and its implications.
President Donald Trump
Trump: Indecisive or Disingenuous?
Although most of Atlas’s criticism is directed at the seemingly incompetent “troika” of Anthony Fauci, Deborah Birx, and Robert Redfield, he is also highly critical of Trump who in fact supported the policies promoted by the troika, despite occasional tweets seemingly to the contrary. Atlas describes Trump as friendly to him and always agreeing with Atlas in private conversations. Atlas is mystified by Trump’s failure to act on his stated beliefs as shared with Atlas, blaming this both on the troika and various Trump advisers rather than Trump personally. Atlas either failed to consider Trump might be pretending to agree with him or chose not to discuss that possibility in his book.
President Trump is a highly successful businessman at one point deeply involved in the rough and tumble casino industry — even taking over Resorts International, a notorious company with a scandalous past. He has a long history of close personal and business “relationships” with murky, rather iffy characters such as the late attorney Roy Cohn, the late singer Michael Jackson, and the late “hedge fund billionaire” without an actual hedge fund Jeffrey Epstein amongst others. That Trump might be something less than straightforward with Atlas or others does not seem improbable.
The actual voting base of Trump is not Pfizer or Bill Gates/Moderna or other giant companies like Walmart or Safeway, it is small business owners, farmers, and large numbers of working class Americans, many employed by small businesses. Atlas briefly notes that Trump’s FDA commissioner Scott Gottlieb took a lucrative position as a member of the board of directors of Pfizer. Atlas does say he disagreed with Gottlieb strongly, but claims he did not attribute Gottlieb’s positions to a conflict of interest with Pfizer. Preteritio?
President Trump had expressed some vaccine skepticism during the 2016 campaign, even suggesting that vaccines might play a causal role in the dramatic increase in autism in the United States over the last three decades. He apparently did reach out to Democrat vaccine skeptic Robert F. Kennedy Jr to pursue a detailed audit of the seemingly confidential public health databases used by CDC and other agencies to clarify the situation.
Robert F. Kennedy Jr. attributes the sudden reversal on this project during the transition period to a large contribution to the Trump inauguration fund by Pfizer. According to Federal Election Commission (FEC) filings, Pfizer donated $1 million dollars to the 58th Presidential Inaugural Committee on December 22, 2016 (see page 163 of the linked 510 page FEC document).
Pfizer has a long history of criminal activities, including aninternational conspiracyin the 1990s with Archer Daniels Midland and several other companies to fix the price of citric acid (a key ingredient of Coca-Cola amongst other products), lysine, and possibly other food additives.
The lockdown policies have been disastrous for these more ordinary Americans while enriching Amazon and other Big Tech companies, giant retailers such as Walmart and Safeway, and indirectly the vaccine makers like Pfizer. Unrest and opposition to the policies surfaced quickly among President Trump’s base, many of whom, contrary to the Democrat picture of mesmerized cultists, are wary of the flamboyantly sleazy casino magnate turned champion of the common man.
It is not uncommon for politicians to pay lip service to the opinions and policies preferred by their voters while in fact enacting the policies preferred by their campaign contributors and business partners.
Lack of Criticism of Operation Warp Speed
A major weakness of the book is Dr. Atlas’s unreserved enthusiasm and endorsement of Operation Warp Speed and the experimental mRNA based vaccines. Although he does not devote much space to this, it is crystal clear in reading the book. He writes approvingly about the policy to exempt the vaccine makers such as Pfizer and Moderna from liability should the vaccines prove harmful.
Dr. Atlas expresses no concern that vaccines based on the SARS-COV-2 spike protein which bonds to the ACE-2 (angiotensin converting enzyme) receptor and appears to severely disrupt the cardiovascular system, causing the often lethal blood clots reported in some COVID patients, might produce similar cardiovascular problems in vaccinated persons, although he does oppose vaccine mandates and the unscientific ignoring of natural immunity in statements by the “public health” authorities, the troika until recently, and others.
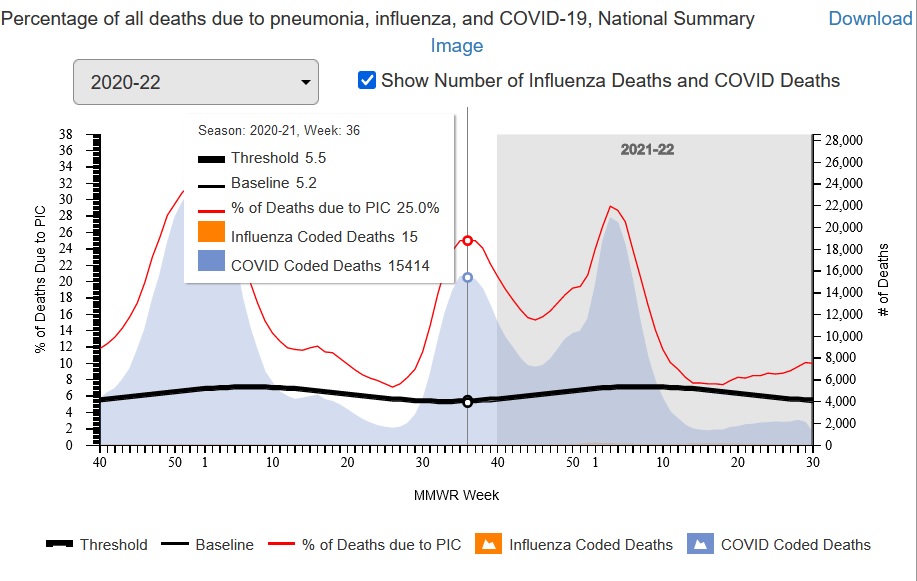
According to the book, Dr. Atlas wrote or completed writing the book in August 2021, arguably just before or as the delta wave was starting to smash through the vaccines, hospitalizing and killing large numbers of Americans if you believe the CDC’s Fluview web site and underlying data as reported.
Vaccine Failure: The COVID-19 “Delta” Wave in August 2021 (about Week 36 of 2021) (US CDC FluView Web Site)
Dr. Atlas expresses no concern about the short circuiting of numerous safety precautions that usually take years to approve a vaccine. Operation Warp Speed met its hyper-aggressive schedule as Atlas proudly claims only by disregarding established safety measures which he does not mention.
In some contexts, usually when making excuses for obvious failures or huge cost and schedule overruns which are common in R&D, scientists such as Dr. Atlas often claim an 80 to 90 percent failure rate for scientific research. For every Manhattan Project that succeeded there are dozens of tokamak fusion power programs, wars on cancer, and so on that have failed. Yet, Dr. Atlas expresses no concerns or fallback plans for the likely failure of Operation Warp Speed if the 80 to 90 percent failure rate is true.
Lack of Self Criticism
Although Dr. Atlas is highly critical of the troika and even President Trump, he does not take himself to task even though he clearly failed to achieve the policies he recommended, citing only a few small successes. This is something of relevance to all of us who seek better policies and to end the irrational hysteria about the COVID pandemic.
Dr. Atlas does claim he was naive about the political process and how politicized the COVID response was. He also is appalled by the censorship, propaganda, and extensive lying or at least false statements by the mainstream media, both “legacy” operations such as the New York Times and social media giants such as YouTube (owned by Google/Alphabet). Other than being outraged, he makes little effort in the book to analyze how and why this is happening and how to successfully combat it.
One may wonder about these claims of naivete given that Dr. Atlas is a fellow at the controversial, mostly conservative Hoover Institution at Stanford University where he has been a health policy analyst for years. The Hoover Institution as a whole is no stranger to bitter partisan political battles.
In any case, Dr. Atlas makes no attempt to understand the crazed “no lie is too big,” “no number of COVID deaths is too many” to GET TRUMP AT ANY COST mentality of the mass media and many others. Indeed this behavior is puzzling and alarming, leading naturally both to psychological explanations such as the “mass formation” theory proposed by Professor Mattias Desmet and grand “conspiracy theories” of varying degrees of seeming plausibility such as those about Klaus Schwab, the World Economic Forum, and the “Great Reset.”
The Collective Fight or Flight Response
Certainly, whether by design (conspiracy) or accident or a mixture of both, we are experiencing a collective fight or flight response on a nearly global scale, a natural response in ancient times when your tribe is attacked by another tribe, in which masks and vaccination are shibboleths to identify friend and foe, like the phrase “lollapalooza” reputedly used by American soldiers in the Pacific during World War II to separate native English speaking US soldiers from Japanese soldiers especially at night.
The collective fight or flight response is the same response that caused massacres of alleged witches, vagabonds, Jews, and others accused of poisoning wells during the Black Death. The fight or flight response is instinctual, overriding higher cognitive functions. High intelligence and formal education does not prevent it or increase one’s ability to shut it off when it is unwarranted — an overreaction for example. It is hard coded into all or nearly all human beings: rich and poor, ignorant and highly educated, dumb and super-smart.
Social conformity, hostility to dissent, censorship, and propaganda all increase markedly during historical episodes of the collective fight or flight response such as during both World Wars. Because of the demonic imagery associated with the Nazis and the Holocaust, it is easier to see the irrationality of the response in World War I than World War II. It is however an irrational, instinctual response rooted in a direct physical attack by a rival tribe in ancient times, not adapted to even modern wars let alone pandemics.
Trump as the American Hitler
Regardless of the motives of any elite conspiracy, Donald Trump’s surprise victory in 2016 caused a collective fight or flight response based on a deep seated belief in and fear of an “American Hitler,” among many Americans, disproportionately liberal Democrats, an insane, evil demagogue who would capture the votes of hillbillies and other stigmatized mostly poor rural whites and lead the US and the World to destruction.
This frightening archetype is common in US popular culture and serious scholarship, dating back at least to the fears of and historical reactions to William Jennings Bryan and most importantly the crusade against Louisiana Senator Huey Long culminating in Long’s assassination in September of 1935, painting Long as the US equivalent of Hitler.
If you believe Trump is the American Hitler, a secular liberal progressive equivalent of the Antichrist figure of the Book of Revelations, then anything is justified to stop him: lying, cheating, stealing, even advocating policies that will in fact increase deaths during a pandemic to undermine him, particularly given the spectre of global thermonuclear war even though the “American Hitler,” Trump, shows a marked antipathy to global thermonuclear war.
Completely irrational behavior such as trying to stop efforts to make deals with Russia and North Korea becomes justifiable if Trump is the American Hitler. Even loopy ideas like provoking a conflict with nuclear armed super-power Russia over Ukraine (currently in the news) to rally the public and prevent Trump or a Trump successor from returning in the mid-term elections may seem reasonable to otherwise intelligent people. Keep in mind if the Trump Republicans were to gain a super-majority in both houses in the 2022 election, they could in principle invalidate the contested 2020 election and restore Trump in 2022 instead of 2024.
Regardless of how unjustified and perhaps unhinged such beliefs about Trump, potential Trump replacements such as Governor De Santis or Senator Rand Paul, or Trump voters actually are, Dr. Atlas, Trump himself, and others have failed to allay them. Once a group of people or a single person is in the instinctual fight or flight response, reason usually fails until they calm down. It is incumbent upon Dr. Atlas to assess why he failed and how to succeed. This is a major weakness of the book.
Conclusion
A Plague Upon Our House paints an alarming portrait of the US government, President Trump and especially the “troika” of Anthony Fauci, Deborah Birx, and Robert Redfield and their many allies — something of continuing concern given Fauci’s current role in the Biden administration. It is filled with anecdotes suggesting Fauci is either incompetent or something worse.
The book would be stronger and more helpful in the continuing crisis if Dr. Atlas carefully evaluated the reasons for his failure to stop the disastrous policies, inability to reach the public and allay the concerns of frightened “never Trumpers,” and how to succeed now in the continuing crisis.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
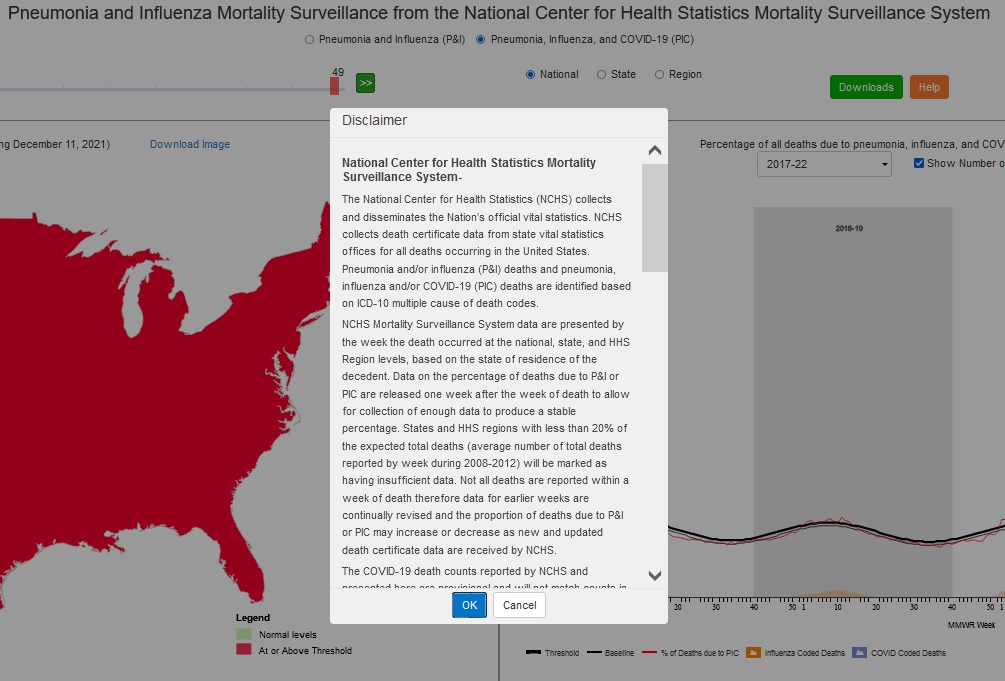
This is the legal disclaimer that appears when starting the US Centers for Disease Control (CDC’s) Fluview Interactive application which purports to report the percentage of deaths per week “due to” pneumonia and influenza (P&I) prior to March 2020 and pneumonia, influenza, and COVID-19 (PIC) since March 2020. (URL: http://gis.cdc.gov/grasp/fluview/mortality.html)
Emphasis is added to key phrases. The NOTES explain the definition and meaning of several technical terms used in the disclaimer.
The disclaimer essentially says, in plain English, the data — the COVID-19 death counts — which is presented with no estimates of statistical or systematic errors is provisional and could be entirely wrong. Two sentences in one paragraph appear to contradict one another.
National Center for Health Statistics Mortality Surveillance System-
NOTE: The National Center for Health Statistics (NCHS) is a division of the US Centers for Disease Control and Prevention (CDC).
The National Center for Health Statistics (NCHS) collects and disseminates the Nation’s official vital statistics. NCHS collects death certificate data from state vital statistics offices for all deaths occurring in the United States. Pneumonia and/or influenza (P&I) deaths and pneumonia, influenza and/or COVID-19 (PIC) deaths are identified based on ICD-10 multiple cause of death codes.
NOTE: ICD-10 is the International Classification of Diseases 10th Edition, a medical classification list by the World Health Organization (WHO). “ICD-10 multiple cause of death codes” refers to multiple “causes of death” listed on death certificates. Many death certificates have many causes of death such as emphysema, a degenerative eventually terminal condition, and pneumonia. One cause of the death is singled out as the “underlying cause of death” or UCOD. One cause of death is singled out as the “immediate cause of death.” The immediate cause of death is often not the underlying cause of death. For example, emphysema may be the underlying cause of death and pneumonia, the influenza virus, or the “common cold” may be the immediate cause of death.
NCHS Mortality Surveillance System data are presented by the week the death occurred at the national, state, and HHS Region levels, based on the state of residence of the decedent. Data on the percentage of deaths due to P&I or PIC are released one week after the week of death to allow for collection of enough data to produce a stable percentage. States and HHS regions with less than 20% of the expected total deaths (average number of total deaths reported by week during 2008-2012) will be marked as having insufficient data. Not all deaths are reported within a week of death therefore data for earlier weeks are continually revised and the proportion of deaths due to P&I or PIC may increase or decrease as new and updated death certificate data are received by NCHS.
NOTE: Notice the conflictbetween “to allow for collection of enough data to produce a stable percentage” and “the proportion of deaths due to P&I or PIC may increase or decrease as new and updated death certificate data are received by NCHS.” Percentage is a way of expressing the proportion: for example, fifty percent (a percentage) versus one half (another way of expressing the same percentage). “Stable” usually means “not changing or fluctuating” (Merriam Webster) when used in this way.
The COVID-19 death counts reported by NCHS and presented here are provisional and will not match counts in other sources, such as media reports or numbers from county health departments. COVID-19 deaths may be classified or defined differently in various reporting and surveillance systems. Death counts reported by NCHS include deaths that have COVID-19 listed as a cause of death and may include laboratory confirmed COVID-19 deaths and clinically confirmed COVID-19 deaths. Provisional death counts reported by NCHS track approximately 1-2 weeks behind other published data sources on the number of COVID-19 deaths in the U.S. These reasons may partly account for differences between NCHS reported death counts and death counts reported in other sources.
NOTE: The language “a cause of death” likely means that COVID-19 (or pneumonia or influenza in pre-2020 figures) is one of the causes of death listed on the death certificate, not necessarily the underlying cause of death (UCOD). Remember, many death certificates have multiple causes of death, one of which is identified as the underlying cause of death. (UCOD). Note also that the disclaimer specifically states that NCHS numbers “will not match..numbers from county health departments.” County health departments are presumably official, primary sources of death data with qualified staff — medical examiners and others.
In previous seasons, the NCHS surveillance data were used to calculate the percent of all deaths occurring each week that had pneumonia and/or influenza (P&I) listed as a cause of death. Because of the ongoing COVID-19 pandemic, COVID-19 coded deaths were added to P&I to create the PIC (pneumonia, influenza, and/or COVID-19) classification. PIC includes all deaths with pneumonia, influenza, and/or COVID-19 listed on the death certificate. Because many influenza deaths and many COVID-19 deaths have pneumonia included on the death certificate, P&I no longer measures the impact of influenza in the same way that it has in the past. This is because the proportion of pneumonia deaths associated with influenza is now influenced by COVID-19-related pneumonia. The PIC percentage and the number of influenza and number of COVID-19 deaths will be presented in order to help better understand the impact of these viruses on mortality and the relative contribution of each virus to PIC mortality.
The PIC percentages are compared to a seasonal baseline of P&I deaths that is calculated using a periodic regression model that incorporates a robust regression procedure applied to data from the previous five years. An increase of 1.645 standard deviations above the seasonal baseline of P&I deaths is considered the “epidemic threshold,” i.e., the point at which the observed proportion of deaths is significantly higher than would be expected at that time of the year in the absence of substantial influenza, and now COVID-related mortality. Baselines and thresholds are calculated at the national and regional level and by age groups.
* The 10 U.S. Department of Health and Human Services regions include the following jurisdictions. Region 1: Connecticut, Main, Massachusetts, New Hampshire, Rhode Island, and Vermont; Region 2: New Jersey, New York, and New York City; Region 3: Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, and West Virginia; Region 4: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee; Region 5: Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin; Region 6: Arkansas, Louisiana, New Mexico, Oklahoma, and Texas; Region 7: Iowa, Kansas, Missouri, and Nebraska; Region 8: Colorado, Montana, North Dakota, South Dakota, Utah, and Wyoming; Region 9: Arizona, California, Hawaii, and Nevada; Region 10: Alaska, Idaho, Oregon, and Washington.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).














{kind=link}