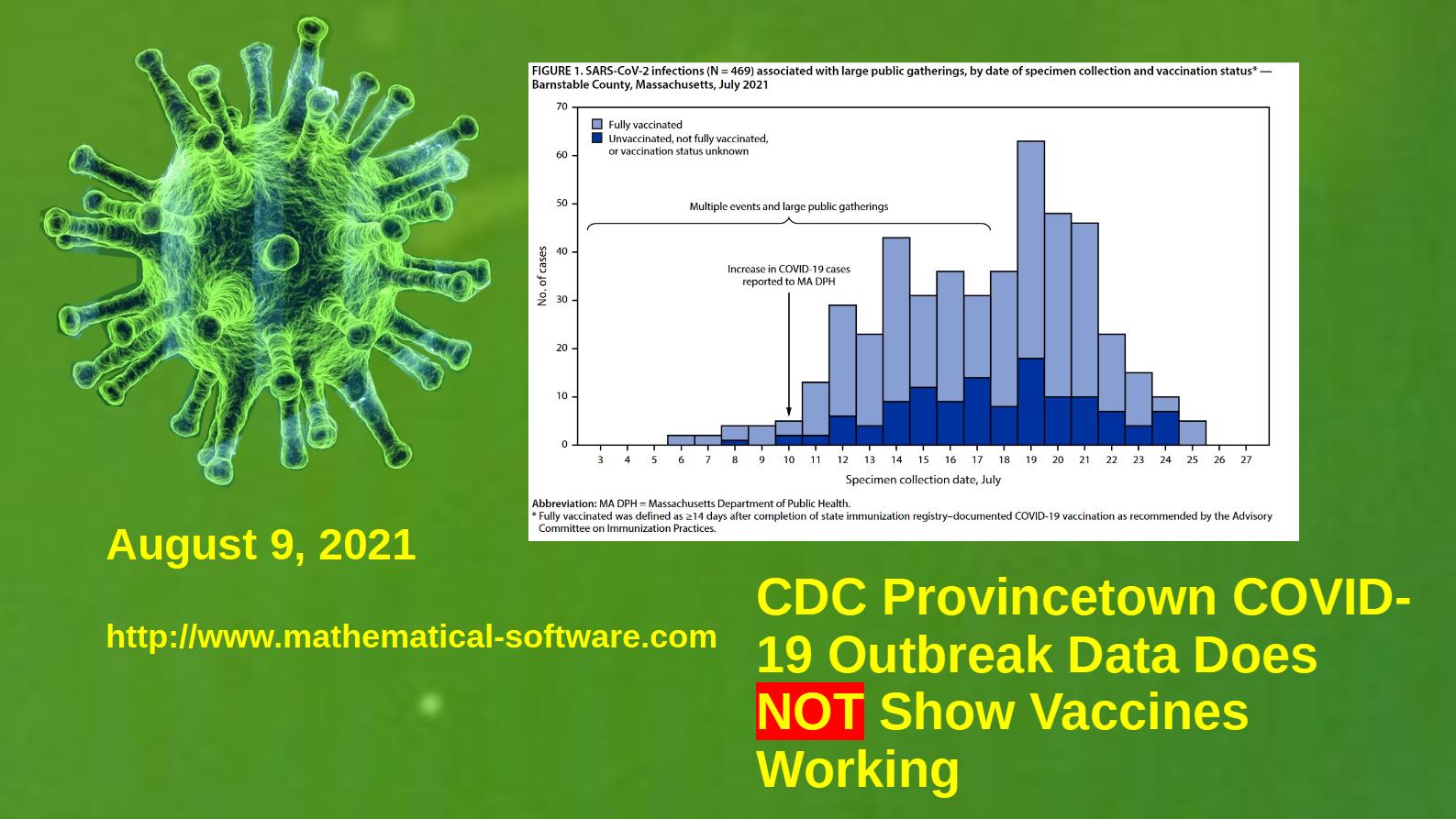
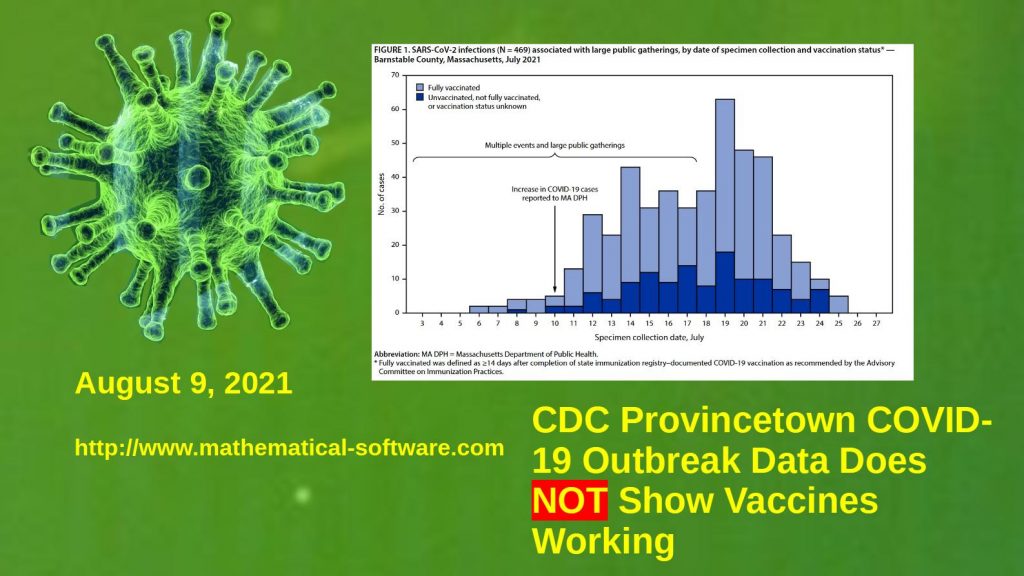
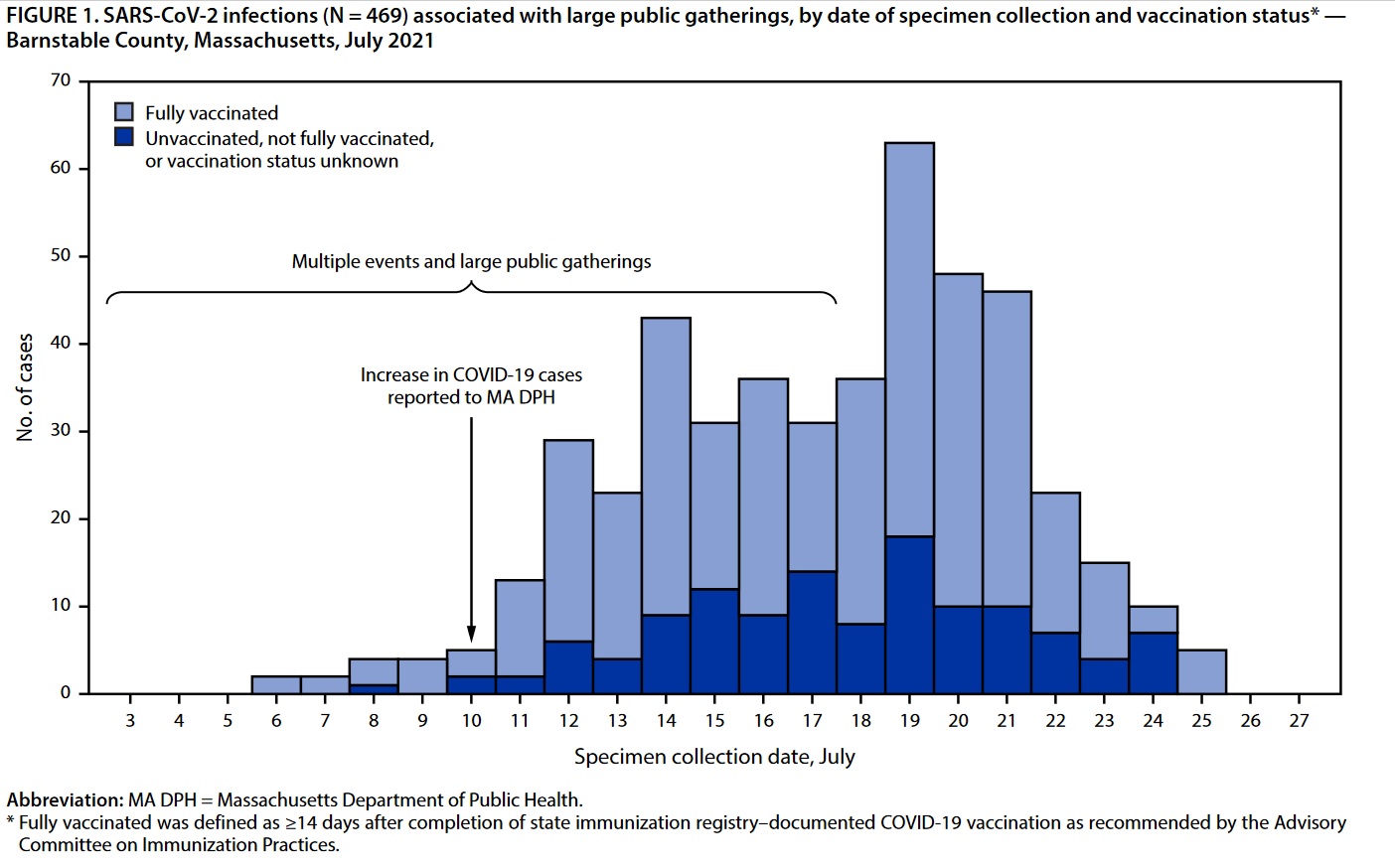
The Provincetown, Massachusetts (Cape Cod, Barnstable County) COVID-19 outbreak does NOT prove that the COVID-19 vaccines are working as widely claimed in the mainstream media. (See the CDC Report “Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings — Barnstable County, Massachusetts,” https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf)
Media reports have often claimed that because no deaths were reported during the outbreak this proves the COVID-19 vaccines work. These media reports often make a comparison to deaths in January of 2021 when widespread vaccination began without actually citing or discussing estimates of the infection fatality rate (IFR) of COVID-19, let alone discussing the seasonality of the infection fatality rate of respiratory diseases.
Note that the infection fatality rate (IFR) of a disease is different from the case fatality rate (CFR) often reported in the mass media, sometimes as several percent for COVID-19 cases. The Case Fatality Rate is generally much larger than the infection fatality rate for many diseases and for COVID-19. Even medical experts who should know better mistakenly conflate CFR and IFR. IFR includes unreported and asymptomatic “cases” whereas CFR does not, hence the lower rate.
Both CFR and IFR can be difficult to compute, estimate, and compare because of varying definitions of “cases” and properly identifying the number of unreported cases with actual symptoms and asymptomatic infections. The COVID-19 pandemic has involved rapidly changing case definitions and poorly validated tests (PCR, antigen, antibody, and even other experimental tests).
Because the CDC was able to identify asymptomatic cases during the Provincetown outbreak, the IFR should be used to evaluate the published data, although the CDC may have missed some, possibly many asymptomatic cases.
Overall, 274 (79%) vaccinated patients with breakthrough infection were symptomatic.
CDC Report, Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings — Barnstable County, Massachusetts, July 2021, Page 1
Similar claims that the outbreak proves the vaccines work have been made regarding the COVID-19 outbreak in heavily vaccinated Israel, so far involving a large fraction of vaccinated persons — often reported as 95% of the COVID-19 cases in Israel.
The CDC Provincetown, Massachusetts (Barnstable County, Cape Cod) data is analyzed in detail below.
According to the CDC report, 469 Massachusetts residents were identified with COVID-19 attributed to attending public events in “a town in Barnstable County, Massachusetts.” This is Provincetown on Cape Cod (Barnstable County, MA is Cape Cod). Of these, 346 (about 74 %) had been fully vaccinated with COVID-19 vaccines: both shots of the Moderna vaccine, both shots of the Pfizer vaccine, and the one shot J&J vaccine at least 14 days prior to infection with COVID-19. One-hundred and twenty-three (about 26 %) were unvaccinated. According to the CDC report, 69% of Massachusetts residents are fully vaccinated against COVID-19. Four fully vaccinated persons were hospitalized and only one unvaccinated person was hospitalized.
The ratio of vaccinated to unvaccinated infected persons (74%) is statistically indistinguishable from the 69% of vaccinated persons in Massachusetts. The most straightforward interpretation of this ratio is that the vaccine failed completely. If the vaccine substantially reduced the risk of infection, we would expect all or most of the cases to be in unvaccinated persons.
It is possible to explain away the ratio of infections by arguing that the vaccinated persons were overconfident, believing the media hype implying the vaccines confer full immunity (“safe and effective” repeated without qualification by most of the mass media). Hence they may have taken risks that spread the disease despite the vaccine, offsetting the benefits of the vaccine. It is clearly remarkable that this exactly offset the effect of the vaccines to produce the same ratio as the fraction of unvaccinated in the general Massachusetts population (the 69%).
The ratio of hospitalized vaccinated to unvaccinated persons (80%) is also statistically indistinguishable from the 69% of vaccinated persons in Massachusetts. The implied hospitalization rate of the vaccinated is 1.16% The implied hospitalization rate of the unvaccinated is only 0.81%. The hospitalization rates are statistically equivalent. Hospitalization is an imperfect proxy for severity of the disease. Consequently, the reported data do NOT show that the vaccines reduced the severity of the COVID-19 disease, contrary to claims by the US CDC, mainstream media, and others.
It is harder to explain away the hospitalizations, a proxy for serious COVID-19. The data gives statistically the same hospitalization rate for vaccinated and unvaccinated persons once infected. Again, however, one could argue the unvaccinated are healthier than the vaccinated to explain the absence of a preponderance of hospitalizations in the unvaccinated. In other words, very healthy persons are correctly less worried about handling a COVID-19 infection without the vaccine and refrain from taking the experimental, largely untested vaccine at this time.
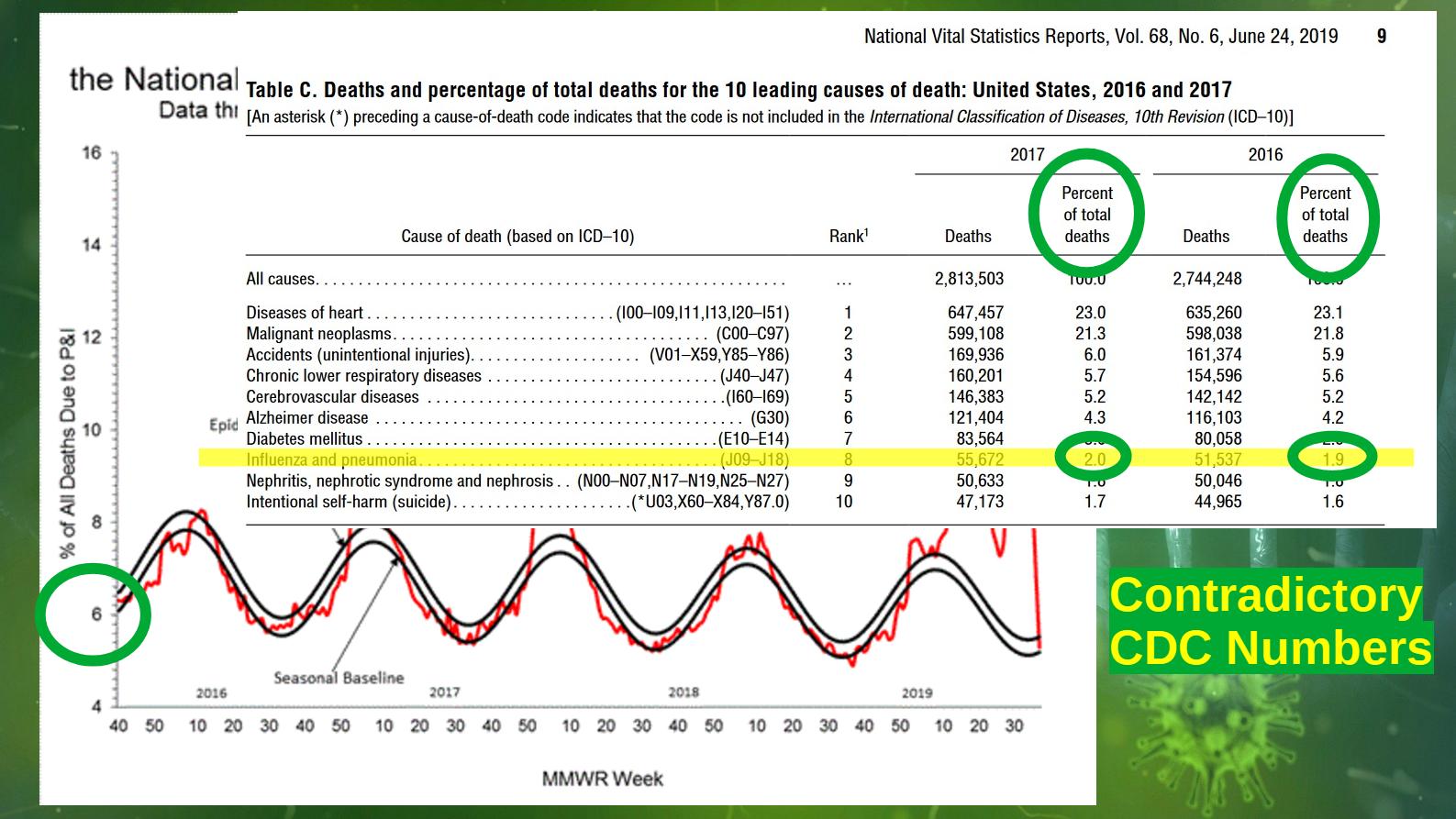
The infection fatality rate (IFR) of COVID-19 (see — for example — https://www.who.int/bulletin/volumes/99/1/20-265892.pdf, https://pubmed.ncbi.nlm.nih.gov/33289900/) is generally estimated as only a few tenths of a percent for “young” (under 70) healthy persons — most of this in persons over 40. The Provincetown COVID-19 outbreak involved July 4th holiday party-goers, generally a young, healthy group. Using an IFR of 0.3%, we might naively expect about 1.2 deaths on average with an uncertainty of 1 death. Hence the absence of even one death in the Provincetown data is hardly surprising and does NOT show that the vaccines are working — even without considering the seasonality of respiratory diseases.
The incidence and mortality of respiratory diseases is seasonal with more infections, cases, hospitalizations, and death in January than in July. The reasons for this pattern are not understood, although it is often attributed to spread of the diseases among school-children in the United States. The sinusoidal — pendulum-like — variation shows no sign of a step up when school opens in the fall or a step down when schools close in the spring/early summer. The pattern suggests the variation is directly or indirectly driven by the Sun.
A number of causes for the seasonality of respiratory diseases have been suggested including vitamin D — which is involved in the immune system — production by sunlight, destruction of the respiratory disease causing organisms by sunlight and specifically the UV light in sunlight, unexplained benefits of sunlight other than vitamin D production, less energy diverted to staying warm when the Sun is stronger, and lower absolute humidity during the cold winter in many regions (NOT ALL) causing longer persistence in the atmosphere of aerosol particles with viruses and sometimes bacteria. In 2020, the COVID outbreak was highly seasonal in most nations with the exception of a surge in the summer in parts of the United States, possibly associated with the George Floyd/Black Lives Matter mass protests.
In conclusion, the CDC’s Provincetown COVID-19 outbreak data does NOT show the vaccines are working — to reduce infections, reduce severity of the disease, or prevent death. The statistics for serious cases of COVID-19 in both the unvaccinated and vaccinated persons are quite small — only five persons (four fully vaccinated, one unvaccinated) hospitalized and no deaths. The lack of deaths is not surprising given the low infection fatality rate (IFR) of COVID-19. Much larger statistics are needed to properly estimate any benefits or harms from the vaccines.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).