
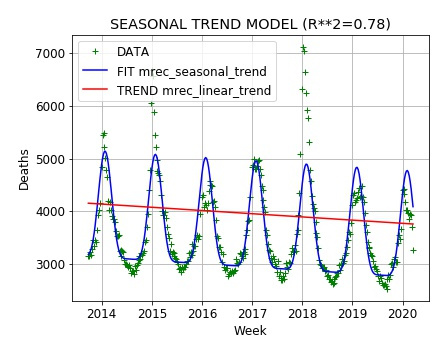
A key question about pneumonia and influenza (including the COVID-19 Sars-Cov-2 coronavirus disease) is the role of weather and temperature on the incidence, severity, and mortality rates from the diseases. Pneumonia and influenza cases and deaths are seasonal, peaking in the winter when sunlight levels and temperatures are lower. The curve for pneumonia and influenza deaths is roughly sinusoidal, which would be expected from something connected to sunlight levels. This is not what one would naively expect from children spreading the disease during the school year; we would expect an abrupt step up in the fall when kids return to school and a step down in the spring when school closes.
A previous post listed a number of resources on the possible direct effects of sunlight through vitamin D production and direct destruction of viruses and bacteria by sunlight, especially the ultraviolet component.
There is a fair amount of research on the role of weather and temperature in the incidence, severity and mortality of pneumonia and influenza. Generally the research seems to support a positive correlation between lower temperatures and also rapid changes in temperature with higher incidence, severity and mortality from pneumonia and influenza as well as other causes of death, notably coronary disease. It also suggests extreme heat “heat waves” is positively correlated with pneumonia. Below are several scientific and scholarly articles; the interested reader can find more articles and details at PubMed (enter “pneumonia and weather” for example in the search box).
Note that correlation does not prove causation.
Scientific and Scholarly Articles
The Lancet
Volume 315, Issue 8183, 28 June 1980, Pages 1405-1408
Journal home page for The Lancet
Occasional Survey
THE WEATHER AND DEATHS FROM PNEUMONIA
Author links open overlay panelG.M.Bull
https://doi.org/10.1016/S0140-6736(80)92666-5
URL: https://www.sciencedirect.com/science/article/pii/S0140673680926665
=============================
Age Ageing. 1978 Nov;7(4):210-24.
Environment, temperature and death rates.
Bull GM, Morton J.
Abstract
Analysis of recorded monthly deaths in England and Wales shows a close association of death rates with external temperature in most diseases other than the cancers. Analysis of daily deaths in England and Wales and in New York shows the following relationships between temperature and deaths from myocardial infarction, strokes and pneumonia. Between -10 degrees and +20 degrees C mimimum temperature there is a nearly linear fall in deaths as the temperature rises. Above 20 degrees C deaths rise steeply as the temperature rises and below -10 degrees C rise steeply as temperature falls. These associations of deaths with temperature are much stronger in the elderly than in younger subjects. Detailed analysis of the daily deaths in England and Wales from myocardial infarction, strokes and pneumonia show that short-term (1–2 days) temperature changes have little effect on death rates but medium-term (7–10 days) and longer-term (three or more weeks) changes associated with very significant changes in death rates. The three diseases vary in the time relations between temperature change and change in death rates. In all three there is an interval between the change in temperature and death and this is shortest in the case of myocardial infarction (1–2 days before death), longest in the case of pneumonia (about a week before death) and intermediate in the case of strokes (about 3–4 days before death). At low temperatures death rates increase as the duration of temperature change increases, while at high temperatures (but below +20 degrees C) death rates decrease as the period of temperature change is longer. The implications of these findings are discussed and it is postulated that there is probably causal relationship between temperature change and deaths from a wide variety of diseases. A proximal link in the chain is probably a failure of autonomic control of body temperature in the elderly leading to a change in body temperature and some humoral change which in turn leads to death. It is not appropriate to concentrate on hypothermia as the relationship between temperature and death is seen at all temperatures.
PMID:
727071
DOI:
10.1093/ageing/7.4.210
[Indexed for MEDLINE] URL: https://www.ncbi.nlm.nih.gov/pubmed/727071
=================================================
Age Ageing. 1975 Feb;4(1):19-31.
Seasonal and short-term relationships of temperature with deaths from myocardial and cerebral infarction.
Bull GM, Morton J.
Abstract
In subjects over 60, changes in temperature lasting two or more days are associated with highly significant changes in death rates from myocardial infarction and cerbral vascular accidents. In both cases, the lower the temperature the higher the death rate and vice versa. Moreover the temperatures one to four days prior to the clinical onset of infarction are more relevant than that on the day of onset, a fact which may have a bearing on prophylaxis. In the case of strokes, a high temperature on the day of onset is also associated with an increase in deaths on that day. The relevance of these findings to possible mechanisms and prophylaxis is discussed.
PMID:
1155294
DOI:
10.1093/ageing/4.1.19
URL: https://www.ncbi.nlm.nih.gov/pubmed/1155294
===========================================
Cardiovascular deaths in winter.
Baghurst PA.
Lancet. 1979 May 5;1(8123):982-3. No abstract available.
PMID:
87658
- J Intern Med. 1991 Dec;230(6):479-85.
High coronary mortality in cold regions of Sweden.
Gyllerup S(1), Lanke J, Lindholm LH, Scherstén B.
Author information:
(1)Health Sciences Centre, Lund University, Dalby, Sweden.
The hypothesis that cold climate is associated with high coronary mortality in
Sweden is tested. Cold exposure was calculated in each of the 284 municipalities
of Sweden. There was a significant association between cold exposure and coronary
mortality in both sexes in all age groups. The strongest association was found in
men aged 40-64 years (coefficient of determination k = 0.39). The decile of men
aged 40-64 years who lived in the coldest municipalities had a 40% excess
mortality. A significant association was also found between cold exposure and
mortality from cerebrovascular diseases. We conclude that there is a strong
regional association between cold exposure and high coronary mortality.
DOI: 10.1111/j.1365-2796.1991.tb00478.x
PMID: 1748856 [Indexed for MEDLINE]
URL (text): https://www.ncbi.nlm.nih.gov/pubmed/11209661
URL (html): https://www.ncbi.nlm.nih.gov/pubmed/1748856
=========================================
- Int J Circumpolar Health. 2000 Oct;59(3-4):160-3.
Cold climate and coronary mortality in Sweden.
Gyllerup S(1).
Author information:
(1)Husensjö Group Practice, Helsingborg, Sweden.
In many European countries there is a tendency towards higher coronary mortality
in the northern parts of the country. Furthermore the highest coronary mortality
rates are found in the colder parts of Europe. We studied the regional variation
in coronary mortality in the 284 Swedish municipalities during a ten-year period
and the relation to the cold exposure in each municipality during the same time
period.METHODS: Mortality rates for each municipality were acquired from the
death certificates and indirectly standardised against the country. Temperature
readings from measurements 5 times a day during daytime were used to form a cold
index. We also compensated for wind chill by using Siples wind chill index.
Multiple regression models were used. Second degree polynomials were used for the
explanatory variables.
RESULTS: There was a strong relation between the cold exposure in a municipality
and coronary mortality. The cold index alone could explain 39% of the regional
variation in coronary mortality. In a multiple regression model, cold index was
the strongest explanatory variable. The coronary mortality in the coldest decile
of the population was 40% higher than in the country as a whole.
CONCLUSIONS: There is a strong regional association between cold exposure and
coronary mortality in Sweden. However, in this type of study, it is not possible
to determine whether this association is a causal one or not.
PMID: 11209661 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/11209661
===========
- Scott Med J. 1993 Dec;38(6):169-72.
Cold climate is an important factor in explaining regional differences in
coronary mortality even if serum cholesterol and other established risk factors
are taken into account.
Gyllerup S(1), Lanke J, Lindholm LH, Schersten B.
Author information:
(1)Health Sciences Centre, Lund University, Dalby Sweden.
Earlier studies have shown a strong regional association between cold climate and
coronary mortality in Sweden and that coronary mortality is more strongly
associated with cold climate than with other explanatory factors such as drinking
water hardness, socioeconomic factors, tobacco and sales of butter. To examine
the joint impact of these factors and to investigate regional differences in
serum cholesterol and their relation to cold climate and coronary mortality,
regression analyses were performed with 259 municipalities in Sweden as units.
Mortality from acute myocardial infarction in men aged 40-64 during 1975-1984 was
used as the dependent variable. A cold index was calculated, this index and the
above mentioned factors were used as explanatory variables. The main results
were: Cold index was the strongest factor when introduced into a multiple
regression model. Four other strong factors had to be used to obtain the same
explanatory strength as cold index did alone, and even when introduced as the
last factor, cold index increased the coefficient of determination substantially.
In a subsample of 37 municipalities, serum cholesterol was not significantly
associated with coronary mortality. However, there was a significant correlation
between cold index and serum cholesterol.
DOI: 10.1177/003693309303800604
PMID: 8146634 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/8146634
======
- Am J Epidemiol. 2016 Oct 15;184(8):555-569. Epub 2016 Oct 6.
Pneumonia Hospitalization Risk in the Elderly Attributable to Cold and Hot
Temperatures in Hong Kong, China.
Qiu H, Sun S, Tang R, Chan KP, Tian L.
The growth of pathogens potentially relevant to respiratory tract infection may
be triggered by changes in ambient temperature. Few studies have examined the
association between ambient temperature and pneumonia incidence, and no studies
have focused on the susceptible elderly population. We aimed to examine the
short-term association between ambient temperature and geriatric pneumonia and to
assess the disease burden attributable to cold and hot temperatures in Hong Kong,
China. Daily time-series data on emergency hospital admissions for geriatric
pneumonia, mean temperature, relative humidity, and air pollution concentrations
between January 2005 and December 2012 were collected. Distributed-lag nonlinear
modeling integrated in quasi-Poisson regression was used to examine the
exposure-lag-response relationship between temperature and pneumonia
hospitalization. Measures of the risk attributable to nonoptimal temperature were
calculated to summarize the disease burden. Subgroup analyses were conducted to
examine the sex difference. We observed significant nonlinear and delayed
associations of both cold and hot temperatures with pneumonia in the elderly,
with cold temperatures having stronger effect estimates. Among the 10.7% of
temperature-related pneumonia hospitalizations, 8.7% and 2.0% were attributed to
cold and hot temperatures, respectively. Most of the temperature-related burden
for pneumonia hospitalizations in Hong Kong was attributable to cold
temperatures, and elderly men had greater susceptibility.
© The Author 2016. Published by Oxford University Press on behalf of the Johns
Hopkins Bloomberg School of Public Health. All rights reserved. For permissions,
please e-mail: journals.permissions@oup.com.
DOI: 10.1093/aje/kww041
PMID: 27744405 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/27744405
============================================================================
- Influenza Other Respir Viruses. 2016 Jul;10(4):310-3. doi: 10.1111/irv.12369.
Epub 2016 May 17.
Cold, dry air is associated with influenza and pneumonia mortality in Auckland,
New Zealand.
Davis RE(1), Dougherty E(1), McArthur C(2), Huang QS(3), Baker MG(4).
Author information:
(1)Department of Environmental Sciences, University of Virginia, Charlottesville,
VA, USA.
(2)Auckland City Hospital, Auckland, New Zealand.
(3)Institute of Environmental Science and Research, Wellington, New Zealand.
(4)University of Otago-Wellington, Wellington, New Zealand.
The relationship between weather and influenza and pneumonia mortality was
examined retrospectively using daily data from 1980 to 2009 in Auckland, New
Zealand, a humid, subtropical location. Mortality events, defined when mortality
exceeded 0·95 standard deviation above the mean, followed periods of anomalously
cold air (ta.m. = -4·1, P < 0·01; tp.m. = -4·2, P < 0·01) and/or anomalously dry
air (ta.m. = -4·1, P < 0·01; tp.m. = -3·8, P < 0·01) by up to 19 days. These
results suggest that respiratory infection is enhanced during unusually cold
conditions and during conditions with unusually low humidity, even in a
subtropical location where humidity is typically high.
© 2015 The Authors. Influenza and Other Respiratory Viruses Published by John
Wiley & Sons Ltd.
DOI: 10.1111/irv.12369
PMCID: PMC4910181
PMID: 26681638 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/26681638
====================================
- Environ Res. 2019 Feb;169:139-146. doi: 10.1016/j.envres.2018.10.031. Epub 2018
Oct 30.
Impacts of cold weather on emergency hospital admission in Texas, 2004-2013.
Chen TH(1), Du XL(1), Chan W(2), Zhang K(3).
Author information:
(1)Department of Epidemiology, Human Genetics and Environmental Sciences, School
of Public Health, The University of Texas Health Science Center at Houston,
Houston, TX 77030, USA.
(2)Department of Biostatistics and Data Science, School of Public Health, The
University of Texas Health Science Center at Houston, Houston, TX, USA.
(3)Department of Epidemiology, Human Genetics and Environmental Sciences, School
of Public Health, The University of Texas Health Science Center at Houston,
Houston, TX 77030, USA; Southwest Center for Occupational and Environmental
Health, School of Public Health, The University of Texas Health Science Center at
Houston, Houston, TX, USA. Electronic address: kai.zhang@uth.tmc.edu.
Cold weather has been identified as a major cause of weather-related deaths in
the U.S. Although the effects of cold weather on mortality has been investigated
extensively, studies on how cold weather affects hospital admissions are limited
particularly in the Southern United States. This study aimed to examine impacts
of cold weather on emergency hospital admissions (EHA) in 12 major Texas
metropolitan statistical areas (MSAs) for the 10-year period, 2004-2013. A
two-stage approach was employed to examine the associations between cold weather
and EHA. First, the cold effects on each MSA were estimated using distributed lag
non-linear models (DLNM). Then a random effects meta-analysis was applied to
estimate pooled effects across all 12 MSAs. Percent increase in risk and
corresponding 95% confidence intervals (CIs) were estimated as with a 1 °C (°C)
decrease in temperature below a MSA-specific threshold for cold effects.
Age-stratified and cause-specific EHA were modeled separately. The majority of
the 12 Texas MSAs were associated with an increased risk in EHA ranging from 0.1%
to 3.8% with a 1 ⁰C decrease below cold thresholds. The pooled effect estimate
was 1.6% (95% CI: 0.9%, 2.2%) increase in all-cause EHA risk with 1 ⁰C decrease
in temperature. Cold wave effects were also observed in most eastern and southern
Texas MSAs. Effects of cold on all-cause EHA were highest in the very elderly
(2.4%, 95% CI: 1.2%, 3.6%). Pooled estimates for cause-specific EHA association
were strongest in pneumonia (3.3%, 95% CI: 2.8%, 3.9%), followed by chronic
obstructive pulmonary disease (3.3%, 95% CI: 2.1%, 4.5%) and respiratory diseases
(2.8%, 95% CI: 1.9%, 3.7%). Cold weather generally increases EHA risk
significantly in Texas, especially in respiratory diseases, and cold effects
estimates increased by elderly population (aged over 75 years). Our findings
provide insight into better intervention strategy to reduce adverse health
effects of cold weather among targeted vulnerable populations.
Copyright © 2018 Elsevier Inc. All rights reserved.
DOI: 10.1016/j.envres.2018.10.031
PMID: 30453131 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/30453131
===========================
- Environ Res. 2014 Jul;132:334-41. doi: 10.1016/j.envres.2014.04.021. Epub 2014
May 14.
Impact of temperature on childhood pneumonia estimated from satellite remote
sensing.
Xu Z(1), Liu Y(2), Ma Z(2), Li S(3), Hu W(1), Tong S(4).
Author information:
(1)School of Public Health and Social Work & Institute of Health and Biomedical
Innovation, Queensland University of Technology, Brisbane, QLD, Australia.
(2)Rollins School of Public Health, Emory University, Atlanta, GA, United States.
(3)School of Public Health, Shanghai Jiaotong University School of Medicine,
Shanghai, China.
(4)School of Public Health and Social Work & Institute of Health and Biomedical
Innovation, Queensland University of Technology, Brisbane, QLD, Australia.
Electronic address: s.tong@qut.edu.au.
The effect of temperature on childhood pneumonia in subtropical regions is
largely unknown so far. This study examined the impact of temperature on
childhood pneumonia in Brisbane, Australia. A quasi-Poisson generalized linear
model combined with a distributed lag non-linear model was used to quantify the
main effect of temperature on emergency department visits (EDVs) for childhood
pneumonia in Brisbane from 2001 to 2010. The model residuals were checked to
identify added effects due to heat waves or cold spells. Both high and low
temperatures were associated with an increase in EDVs for childhood pneumonia.
Children aged 2-5 years, and female children were particularly vulnerable to the
impacts of heat and cold, and Indigenous children were sensitive to heat. Heat
waves and cold spells had significant added effects on childhood pneumonia, and
the magnitude of these effects increased with intensity and duration. There were
changes over time in both the main and added effects of temperature on childhood
pneumonia. Children, especially those female and Indigenous, should be
particularly protected from extreme temperatures. Future development of early
warning systems should take the change over time in the impact of temperature on
children’s health into account.
Copyright © 2014 Elsevier Inc. All rights reserved.
DOI: 10.1016/j.envres.2014.04.021
PMID: 24834830 [Indexed for MEDLINE]
URL: https://www.ncbi.nlm.nih.gov/pubmed/24834830
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).