
In coverage of the coronavirus COVID-19 pandemic, one often sees a value for the infection fatality rate (also known as the actual mortality rate, which is different from the “case fatality rate”) of 0.1 percent, meaning one in 1000 people infected by the “flu” dies. Infected includes people who are asymptomatic, have mild cases — anyone who is actually infected even if never detected. It is often explicitly or implicitly argued that if the infection fatality rate of COVID-19 is only 0.1 percent as suggested by a recent study by Stanford researchers (https://www.medrxiv.org/content/10.1101/2020.04.14.20062463v1.full.pdf) we can relax and go back to work. Unfortunately, it is probably not that simple.
NOTE: Companion video at https://youtu.be/QB4eyDBgxYI and https://www.bitchute.com/video/FCxo6c9LfiIF/ The video is about 32 minutes and includes some longer commentary on some technical points. It is generally faster to read the article than watch the video.
We can use our prevalence estimates to approximate the infection fatality rate from COVID-19 in Santa Clara County. As of April 10, 2020, 50 people have died of COVID-19 in the County, with an average increase of 6% daily in the number of deaths. If our estimates of48,000-81,000 infections represent the cumulative total on April 1, and we project deaths to April 22 (a 3 week lag from time of infection to death22), we estimate about 100 deaths in the county. A hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%. If antibodies take longer than 3 days to appear, if the average duration from case identification to death is less than 3 weeks, or if the epidemic wave has peaked and growth in deaths is less than 6% daily, then the infection fatality rate would be lower. These straightforward estimations of infection fatality rate fail to account for age structure and changing treatment approaches to COVID-19. Nevertheless,our prevalence estimates can be used to update existing fatality rates given the large upwards revision of under-ascertainment
COVID-19 Antibody Seroprevalence in Santa Clara County, California by Bendavid et al
According to the United States Centers for Disease Control (CDC) there are either about 55,000 deaths from “influenza and pneumonia” (from the 2017 leading causes of death: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf, Table B, Page Six) or about 188,000 (from the weekly “pneumonia and influenza” mortality surveillance — see for example: https://www.cdc.gov/flu/weekly/weeklyarchives2019-2020/data/NCHSData14.csv).
Let’s do some very simple calculations.
It is thought the vast majority of adults get at least two symptomatic “colds” or “flus” in common usage (The CDC claims adults get 2-3 “common colds” per year and children more on their web site which matches common experience.). These are caused by a wide variety of viruses and bacteria and sometimes chemical toxins. These include the rhinovirus, various coronaviruses other that the “novel” SARS-COV-2 coronavirus, and many others including a category of viruses known as “influenza” or “influenza viruses”.
With a total US population of about 330 million, we can estimate at least 660 million individual cases and separate infections of these “cold” or “flu” organisms (either viruses or bacteria) each year. This gives a naive effective infection fatality rate averaged over the population and different diseases of:
188,000 divided by 660 million is: 0.028 percent (0.00028484848484848485)
55,000 divided by 660 million is: 0.008 percent (0.00008333333333)
This is of course much less than 0.1 percent (one in 1000).
What gives?
In common English usage, the terms “cold” and “flu” are often used interchangeably. The use of the terms “flu” and “influenza” to describe respiratory illnesses that vary in incidence seasonally predates the discovery of the influenza viruses, a category of viruses that can cause these symptoms. Influenza is Italian, from the Latin “influentia,” for “influence,” referring to the baleful influence of the stars that the ancients blamed for the disease.
The CDC hopelessly blurs the distinctions, if any, between “common cold”, “cold”, “flu”, “influenza”, “influenza like illness,” “influenza associated,” “pneumonia,” and other terms in its promotional and “scientific” materials.
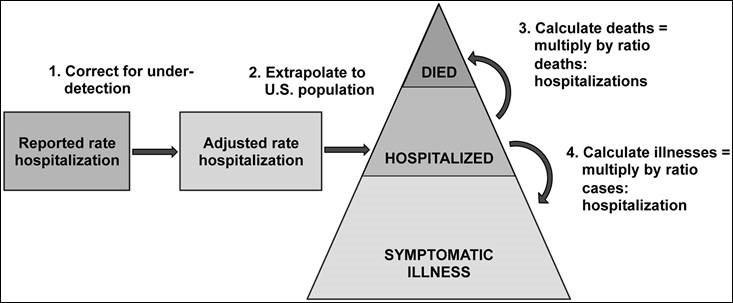
Influenza as in the influenza viruses is rarely listed as a cause of death on death certificates. The weekly “pneumonia and influenza” death numbers from the National Center for Health Statistics (NCHS) only list about 8,000 deaths from influenza in 2017. The CDC cites several different reasons for claiming there is massive underdiagnosis and underreporting of influenza (THE VIRUS) deaths, dating back to at least 2005 and persisting despite the CDC’s extensive educational efforts.
The CDC uses a mysterious model to estimate about 55,000 annual deaths from influenza (THE VIRUS). Presumably the number of deaths from “influenza and pneumonia” in the leading causes of death is this number or something closely related — but this is not clear. Incidentally, in this age of the Internet and pervasive computing, the CDC could publish the actual source code for their model in a free open-source language such as Python on their web site for all to see and review.
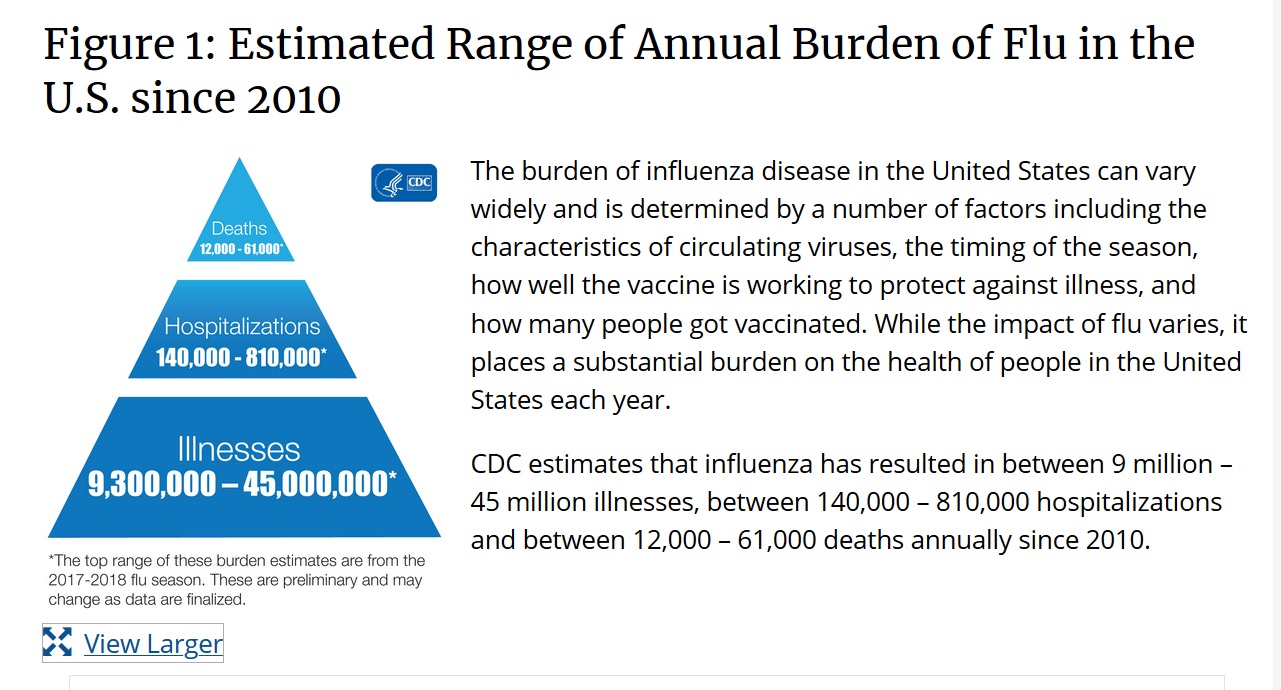
Part of this model is an estimate of how many “colds” are caused by an influenza virus. Presumably this number is about 55 million to get the widely quoted 0.1 percent (one in 1000) infection fatality rate for influenza. This is an example of the CDC’s estimates from https://www.cdc.gov/flu/about/burden/index.html:

Thus, the CDC estimates about 55 million of the annual over 660 million “cold” cases in the United States is caused by “influenza disease” or “influenza” or “flu,” presumably meaning cases caused by influenza viruses. This is probably less than ten percent of all “colds.” The CDC also estimates about 55,000 deaths from influenza viruses. This presumably gives the about 0.1 percent (one in 1000) number widely quoted in the media.
Everyone should understand that a 0.1 percent (one in 1000) infection fatality rate is much higher than the effective infection fatality rate of all the diseases that cause deaths attributed to “pneumonia and influenza” and that also typically cause two “common colds” or “flus” in healthy adults each year.
Even accepting the CDC’s estimates of the prevalence of illness due to influenza viruses (THE VIRUS), less than ten percent of all “common colds,” if the coronavirus COVID-19 spreads more easily than the influenza viruses, it may be able to kill more people than the influenza viruses with the same infection fatality rate (e.g. one in 1000, 0.1 percent). We also need to know how the SARS-COV-2 coronavirus spreads and how quickly.
If everyone in the United States were infected with the COVID-19 coronavirus, a 0.1 percent infection fatality rate (one in 1,000) would probably mean somewhat less than 330,000 additional deaths on top of the roughly 188,000 deaths from “pneumonia and influenza” (or is it 55,000 from “influenza and pneumonia”). There would be some overlap between COVID-19 coronavirus deaths and deaths of susceptible, mostly elderly persons that would have happened anyway due to conventional non-COVID diseases including the influenza viruses.
Conclusion
There is a remarkable lack of key measurements in the current coronavirus COVID-19 pandemic. These include the actual mortality rate (aka infection fatality rate) broken down by age, sex, race, pre-existing medical conditions, ambient temperature, sunlight levels, pollution levels, and other risk factors. The false positive and false negative rates of the tests for the disease, both the tests for an active infection such as the RT-PCR tests and tests for past infection such as the antibody tests. The methods and rates of transmission for the disease. Aerosol transmission probably occurs at least at a low level and is virtually unstoppable.
The CDC and the National Security bioweapons defense programs should have been set up to quickly and efficiently collect these key data and parameters as soon as a possible outbreak or attack was detected, independent of warnings and information provided by a potential adversary such as China or from the World Health Organization (WHO).
The confusing language and numbers on pneumonia and influenza on the CDC web site and in various official reports and documents seem to be primarily for marketing the flu vaccines rather than enabling informed decisions by patients and doctors or supporting external scientific research into the influenza viruses or other diseases.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).