Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The Psychology of Totalitarianism is a new book by Mattias Desmet, a professor of clinical psychology at Ghent University in Belgium, outlining his theory of “mass formation” especially with respect to the response to the COVID-19 pandemic. His theory of “mass formation” was popularized by Dr. Robert Malone, the inventor or one of the inventors of the mRNA vaccine technology, during Malone’s Joe Rogan interview on the COVID pandemic and the COVID vaccines, using the name “mass formation psychosis” which Desmet does not use. Desmet has appeared on several podcasts touting his ideas since then, with several recent appearances to promote the book.
Briefly, I found the case for Desmet’s theory of mass formation with respect to the COVID response unconvincing, although I believe some of the factors such as widespread loneliness and social isolation that he discusses are contributing factors. Some sections of the book are quite interesting and insightful but for other reasons.
Rather, the “groupthink” and grossly irrational behavior during the COVID pandemic can be attributed to a “collective fight or flight response” not specific to totalitarianism, long predating the modern era, and common during wars and war-like episodes such as the aftermath of the September 11 attacks in the United States, World War I and World War II. This collective fight or flight response has been aggravated by pandemic profiteers such as Pfizer and Bill Gates much the same way that “Merchants of Death” selling weapons have aggravated the fight or flight response both before and during wars.
Mass formation is a theory to explain extreme instances of “mass hysteria” or “groupthink” including such episodes as the bloody purges in Stalinist Russia and Nazi Germany. The term and various mass formation theories predates Desmet who has his own variant of the theory which is elaborated in detail in the book. He cites such scholars as Gustave Le Bon and Hannah Arendt.
The book is well written, translated into easily readable English by Els Vanbrabant. A few sections are a bit dry and academic, but overall the English version is clear and interesting with no hint that it is translated other than the frequent references to Belgium and Belgians. It includes an index and references, although a number of critical statements lack footnotes.
The book is clearly marketed toward skeptics of the official COVID narrative or those with significant doubts — hopefully a large and growing group given the evident massive failures of the COVID vaccines since the summer of 2021. Others may be unable to see the case for widespread mass hysteria, groupthink, or other irrationality in the COVID response. The book cover and first pages feature numerous laudatory quotes from Robert Malone MD, Peter McCullough MD, and other prominent critics of the official narrative, policies, and generally the COVID vaccines. These one sided endorsements are likely to limit the reach of the book.
Desmet’s mass formation theory in the book is really two theories that he links together in a whole. The second theory is the mass formation theory that Desmet and Malone have discussed on several occasions. Namely, a general environment of loneliness, social isolation, lack of meaning, and “free floating anxiety” leads to a situation where a large fraction of the population (about thirty percent) fanatically embraces a simplistic, often rapidly changing narrative that provides a powerful sense of both meaning and solidarity with other people, substituting the greater good of the collective for normal social and moral relations. This mass formation is a form of collective hypnosis involving a narrow focus on a single simple goal such as “zero COVID” at any cost, including self-destructive measures and monstrous acts that would normally be rejected as immoral.
A Critique of Scientific “Rationalism”
In the book, Desmet attributes this environment of loneliness, social isolation, lack of meaning, and the associated free floating anxiety to the flaws and limitations of the modern Enlightenment rational materialistic mechanical worldview beloved of many scientists, engineers, and other intellectuals including himself until age thirty-five. Note that the social isolation and associated problems could have another cause than the rational scientific worldview but give rise to the mass formation. Desmet is specific in blaming the “rational” worldview however for the preexisting conditions that make possible the mass formation.
Desmet’s critique of the “rationalist” worldview, perhaps better called “scientism,” is extensive with many good points and insightful discussions of flaws in mainstream science and statistics, making up most of the book, nearly all of the first and third parts. The mass formation theory that many readers may have encountered on podcasts before the book’s recent publication makes up part two which is only about three chapters, sixty pages.
For me Desmet’s extensive criticism of the scientific rationalist materialistic worldview as he calls it was the most interesting part of the book, even though I disagree with his overall thesis. I found his discussion of the practical problems with statistics and graphical data presentation, focusing on the dismal and misleading use of statistics during the COVID pandemic, particularly interesting and insightful.
That said, Desmet’s discussion of quantum mechanics in modern physics is incorrect. The mainstream Copenhagen interpretation of quantum mechanics does not give consciousness any special role in the measurement or observation in quantum mechanics. Some physicists have theorized consciousness in some way is the “measurement” or “observation” that collapses the quantum wave function in the mainstream Copenhagen theory. This is a fringe view.
The Copenhagen interpretation of quantum mechanics is almost certainly “incomplete” and logically flawed as Einstein argued in his 1935 paper with Podolsky and Rosen. The problem is the lack of a clear consistent definition of “measurement” or “observation” in the mainstream theory. Incompleteness does not however mean that consciousness plays a central role in quantum mechanics as Desmet claims in several places. Most non-Copenhagen theories to resolve the incompleteness — for example the many worlds theory of QM — do not use consciousness to resolve the logical flaws in the Copenhagen Quantum Mechanics illustrated by Schrodinger’s Cat and other paradoxes.
David Bohm’s pilot wave theory — derived from the earlier pilot wave ideas of his mentor Einstein as well as deBroglie and Schrodinger — actually removes the need to invoke either a wave function collapse or consciousness by interpreting the quantum system as a pilot wave and a discrete particle somewhat like radar controlled drone guided by a radar signal bouncing and diffracting through a mountain range. The drone always has a specific location and velocity whereas the radar beam is spread out over the landscape, interfering with itself and causing confusing wavelike behavior in the trajectory of the drone.
Although Bohm linked his ideas to mysticism with the pilot wave or “quantum potential” analogized to the World Spirit (Anima Mundi) of western mysticism or the chi of eastern mysticism, the pilot wave theory is entirely mechanistic.
Desmet’s discussion of the supposed scientific revolution during the 17th century, illustrated with the usual stories about Galileo, is what most scientists and intellectuals in the modern world are taught. Yet it is grossly contradicted by the actual historical record which shows a seamless evolution from religion and mysticism, most clearly with the work of Johannes Kepler and Tycho Brahe, both mystics, alchemists, astrologers, and deeply religious men who envisioned God as mathematician dictating mathematical laws obeyed by subsidiary spirits or angels embodied in the Sun and planets.
This notion of a predictable, mathematical universe created by a God or gods is very old, dating back to Pythagoras in ancient Greek and very likely Pythagoras’s teachers in Egypt and Babylonia (modern Iraq). A benevolent God would hardly be the capricious, inscrutable nut case pictured by Carl Sagan and other atheist science popularizers in recent decades, instead providing rational laws of nature for His human creations.
The common textbook notion of a scientific revolution in the 17th century rejecting medieval religion and superstition, epitomized by Galileo and his clash with the Catholic Church, appears to be a projection of atheistic, materialistic views that became dominant in organized, professionalized science during the 19th century and early 20th century.
The Collective Fight or Flight Response
The fight or flight response is a powerful reaction to an immediate perceived threat such as a tiger or other large predator, a car accident, a human antagonist such as a mugger, or other physical dangers. It involves a narrowing of focus to the immediate threat, short term thinking, a strong physical response mediated by adrenaline and other hormones.
An extreme fight or flight response can include loss of pain sensations, the ability to fight and kill with severe, normally disabling or fatal injuries, and other dramatic changes. Many higher cognitive functions are lowered or turned off to handle the immediate threat. Some short term thinking skills and reflexes may be enhanced instead. The immune system is reduced or turned off to focus all energies on the immediate threat.
Human beings and other herd animals also have a collective fight or flight response most evident during wars or public emergencies. Obedience to authority increases. Conformity increases. People and groups that are perceived as different are frequently attacked, isolated (e.g. confinement of American Indians to reservations, internment of Japanese Americans in WW2), driven out (e.g. enslavement and expulsion of most Wampanoag from the Massachusetts colony after King Philips War in 1675) or killed (e.g. massacre of settlers by the Dakota Sioux in Minnesota in 1862). The collective focus narrows to the immediate survival threat. Group members will display flags or other signs to indicate membership in the group (e.g. wearing masks during the COVID pandemic, displaying vaccine cards and certificates) and make differentiating the group from the attackers easier.
These are instinctive, primal responses probably adapted to repelling an attack by a rival tribe or clan in ancient times. As in the individual fight or flight response, higher cognitive function is curtailed or turned off. If your village is being attacked by the tribe across the river, it is not the time for nuanced thought. Language such as “you are either with us or against us” surfaces. The tribe coalesces into a single military unit and fights as one.
The collective fight or flight response does not require preexisting loneliness, social isolation, discontent, a lack of meaning or any negative conditions at all. It simply requires a perceived physical threat to the group.
This is the “mass formation” behavior during the COVID-19 pandemic. Pandemics, even if due to the deliberate release of a biological weapon, are not attacks by a rival tribe in 10,000 BC. The collective fight or flight response can be disastrous in a non-military public emergency, real or imagined.
War profiteers learned a long time ago to provoke and exploit the collective fight or flight response to create and prolong wars, boosting profits often with disastrous consequences for most people. Pandemic profiteers such as Pfizer and Bill Gates can do the same.
Conclusion
The Psychology of Totalitarianism is well worth reading, both because of Desmet’s insights on scientific rationalism and because it will undoubtedly influence the debate and conflict over the COVID pandemic, vaccines, and policies. However, those skeptical of the rapidly changing COVID narrative or major parts of the narrative should not embrace Desmet’s mass formation hypothesis. While it is likely widespread loneliness and lack of meaning has contributed to the overreaction, the main cause is probably the primal collective fight or flight response stoked by a continuing barrage of fear porn from the advertising funded mass media.
Psychoanalyzing people to their face is rarely persuasive. Most people find this condescending and offensive. Desmet eschews the phrase “mass formation psychosis” with good reason and COVID skeptics should particularly avoid telling other people that they are psychotic.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The omicron variant of the SARS-COV-2 virus, widespread testing including the newly available (in US) antigen tests, or some combination of these factors has resulted in a huge number of both cases and deaths attributed to SARS-COV-2 despite widespread vaccination. Cases and deaths have soared in groups and regions such as Israel and the UK reporting very high vaccination rates, making attributing the cases to the “unvaccinated” implausible.
This has put public health authorities such as the US Centers for Disease Control and Prevention (CDC), WHO, and other agencies around the world in a bind. At best, the soaring cases and deaths reflect either extensive failure of the current vaccines or high false positive rates in the various tests resulting in other respiratory disease cases and other deaths being misidentified as COVID-19.
For the sake of argument, accept that the vaccines are quite safe despite the alarming VAERS data in the United States and that, as widely claimed, the vaccines do confer some reduction in death and severity of illness for a brief few month duration, nonetheless the huge number of cases and deaths throughout the world suggests that the vaccines are largely ineffective in real-world conditions. This may be due to omicron mutating around the vaccine induced immunity based on earlier variants of SARS-COV-2, the frequent waning of the immunity conferred by inactivated vaccines, or even other causes not identified.
This failure of course is an embarrassing debacle at best for public health authorities and agencies, political leaders, and various billionaire philanthropists, particularly because the costly and disruptive lockdowns were justified to protect the vulnerable until a life-saving vaccine would be available – despite the well known high failure rate of research and development, often estimated at 80-90 percent.
However, if current omicron cases and deaths reflect high false positive rates, the past case and death counts since March of 2020, often described by public health authorities or mainstream news reports citing unnamed public health authorities when reported as both “undercounts” and highly accurate are even more suspect than recent numbers. In the United States, the CDC has previously explained the lack of real time data reporting and other flaws in the COVID-19 case and death data, causing officials to rely on data from the UK and Israel, as caused by antiquated IT systems, lack of funding in previous budgets, alleged cuts by the Trump administration, and similar excuses.
Many of the early tests were produced in haste, rushed out under experimental use authorizations (EUA), including an embarrassing failure by CDC early in the pandemic to produce a usable PCR test (URL: https://arstechnica.com/science/2020/04/cdcs-failed-coronavirus-tests-were-tainted-with-coronavirus-feds-confirm/ ). Tests, testing methods and technologies should certainly have improved in the last two years of the pandemic; if not, why not? Especially given the trillions of dollars spent on the pandemic response.
Some mainstream reporting on problems with the US CDC’s data and data handling.
The current crisis in the Ukraine has undoubtedly distracted much of the public from the omicron bind. Nonetheless the soaring cases and deaths attributed to the omicron and post-omicron variants of SARS-COV-2 appears to reveal gross contradictions in the claims by public health authorities about the COVID pandemic. While it is usually possible in practice to find some convoluted, acrobatic explanation for obviously contradictory data and/or logic, such explanations are rarely true.
Improper Scientific Practice
The public health authorities are portraying the flip flops and contradictions in their assertions about COVID as brilliant scientific discoveries — new science or the science has changed — although that excuse is wearing thin. This is not how proper science functions — even major breakthroughs. It proceeds from tentative statements and numbers with large error bars and/or broad confidence intervals to smaller and smaller errors as more data, better measurements, and better models are developed.
Error bars are graphical representations of the variability of data and used on graphs to indicate the error or uncertainty in a reported measurement. They give a general idea of how precise a measurement is, or conversely, how far from the reported value the true (error free) value might be. Error bars often represent one standard deviation of uncertainty, one standard error, or a particular confidence interval (e.g., a 95% interval). These quantities are not the same and so the measure selected should be stated explicitly in the graph or supporting text. Error Bars, Wikipedia, March 25, 2022
Science rarely jumps from super-confident statements such as “masks don’t work” to grossly contradictory super-confident statements such as CDC Director Robert Redfield’s ludicrous “masks will stop the pandemic in 8-12 weeks” statements in the summer of 2020. (LINK: https://people.com/health/americans-wore-masks-drive-this-epidemic-to-the-ground-says-cdc-director/ ) That sort of a jump or contradiction usually indicates bad science — gross underestimation of the errors before or after the jump (or both). In most cases, the scientific discovery is reflected in a sharp discontinuous drop in the error bars due to a better theoretical and/or mathematical model or better measurements or both.
For example, Johannes Kepler’s discovery of the elliptical orbits of the planets combined with superior measurements with the new telescopes in the 17th century resulted in a dramatic drop in the error bars on predictions of planetary motions from about a one percent (1%) error with the Ptolemaic system to a tiny fraction of one percent. It did not result in a gross reversal of centuries of astronomical observations and predictions. Ptolemy and his successors knew their model was imperfect and said so. Mars did not suddenly stop backing up for two months every two years in 1605 when Kepler realized what was going on. The empirical phenomenon did not somehow reverse overnight, rather our understanding leaped forward and the accuracy of the predictions went up dramatically.
(ABOVE) The red error bars and the dark blue data points show the ideal proper scientific practice in which the reported red error bars include the actual value largely determined in the 2015-2016 period in the hypothetical example shown when the science jumps forward. The green error bars and light cyan data points show improper scientific practice in which the scientists are over-confident both before and after the “breakthrough.”
It is common for over-confident scientists to explain the contradiction by referring to the uncertainty of science as if the poorly educated audience or critic is unaware of uncertainty and as if the scientists properly reported the large pre-2015 red error bars previously whereas they actually reported the incorrect small green error bars. This switch is the scientific uncertainty excuse.
Indeed there is a frequent improper failure to report statistical and systematic errors throughout the public health “science” both as presented to the lay public, on news shows, and in CDC and other web sites and publications. One of the most striking examples is a large difference in the number of deaths attributed to “pneumonia and influenza” on the US CDC FluView website (~188,000 per year) and the US CDC leading causes of death report (~55,000 per year). These grossly contradictory numbers have been reported for years with no statistical or systematic errors, nor clear explanation for the difference. The discrepancy between the FluView website and the leading causes of death report predates the COVID-19 pandemic by several years. This gross discrepancy is likely extremely relevant to the question whether a death is “with COVID” or “from COVID” or some intermediate case.
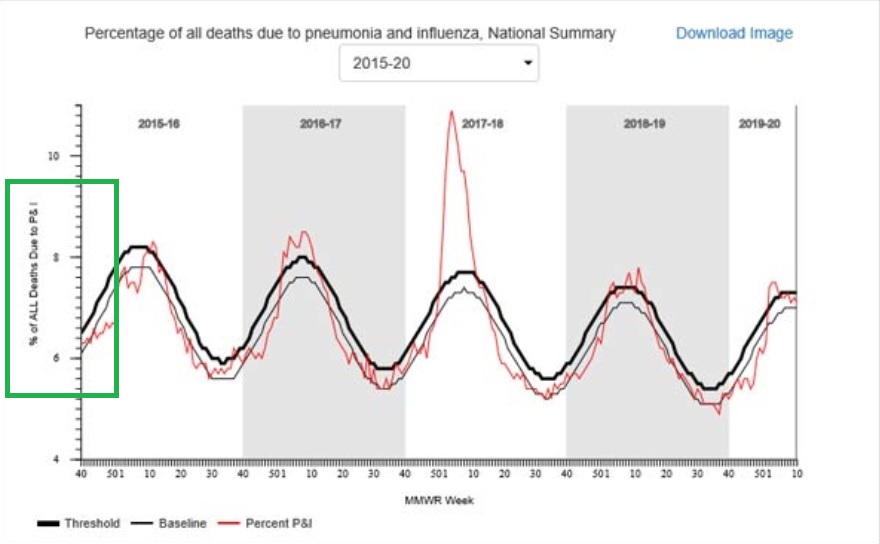
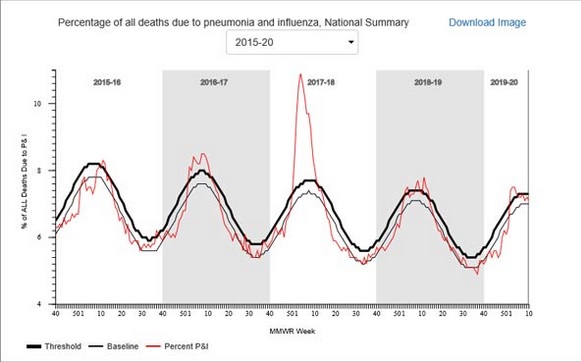
The CDC FluView website shows that 6-10 percent of all deaths, varying seasonally, are due to (the precise language on the graphic) pneumonia and influenza (P&I) according to the vertical axis label on the FluView Pneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list, as mentioned, ~188,000 deaths per year attributed to pneumonia and influenza.
The CDC FluView graphic and underlying data files list no statistical or systematic errors. The counts of deaths in the data files give the numbers to the last significant digit, implying an error of less than one count, one death, based on common scientific and engineering practice.
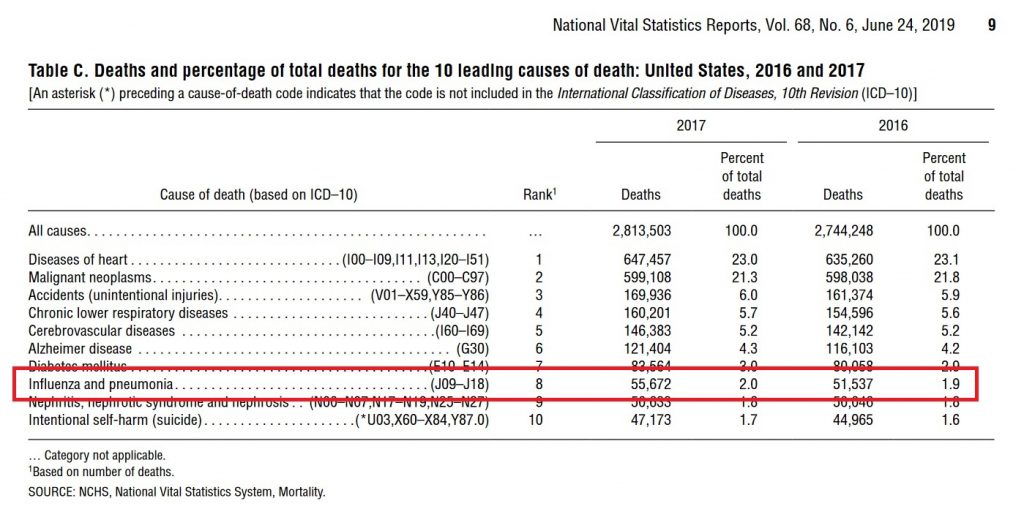
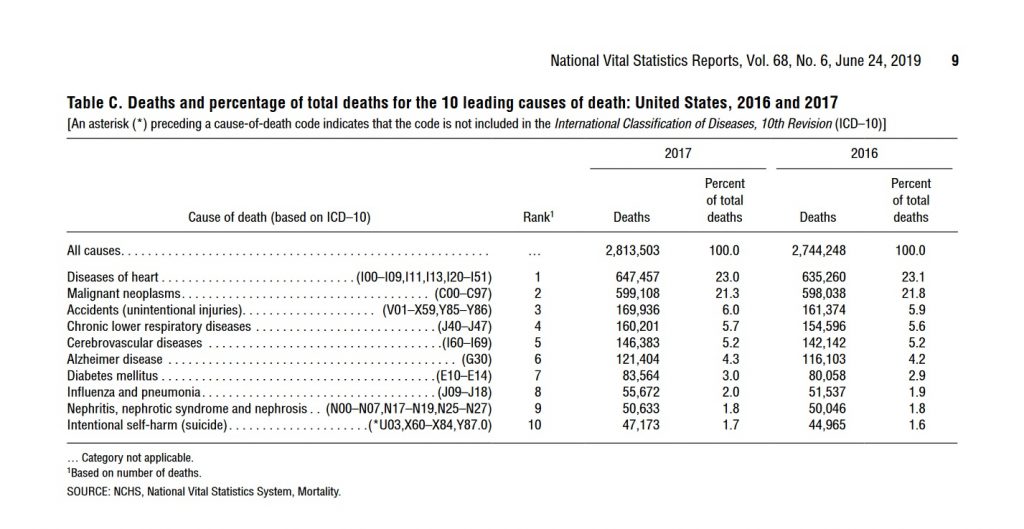
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see Figure 3) attributes only 2 percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers seems to be due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not, however, clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some or even many cases. Despite this, none of these official numbers, either in the leading causes of death report or the FluView website, are reported with error bars or error estimates, as is the common scientific and engineering practice when numbers are uncertain. The leading causes of death report for 2017 reports exactly 55,672 deaths from “influenza and pneumonia” in 2017 with no errors– as shown in Figure 2.
It is impossible to perform an accurate cost benefit analysis of any policy without honest reporting of the uncertainties/error bars. The overconfident statements will have serious real world consequences in human lives unless they prove correct through luck.
Generally statements with — in fact — large error bars should not override personal judgment (e.g. mandates) especially in life and death situations. The government may be justified in preventing parents from treating an illness with a fatal dose of cyanide, where the lethality of the “treatment” is certain. The government is certainly not justified in compelling parents to treat an illness with an experimental treatment with large uncertainties and unknowns even if that treatment might save the child’s life.
Scientists have an ethical obligation to honestly compute and report both statistical and systematic errors; this is common scientific and engineering practice taught by accredited universities and colleges throughout the world.
(C) 2022 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
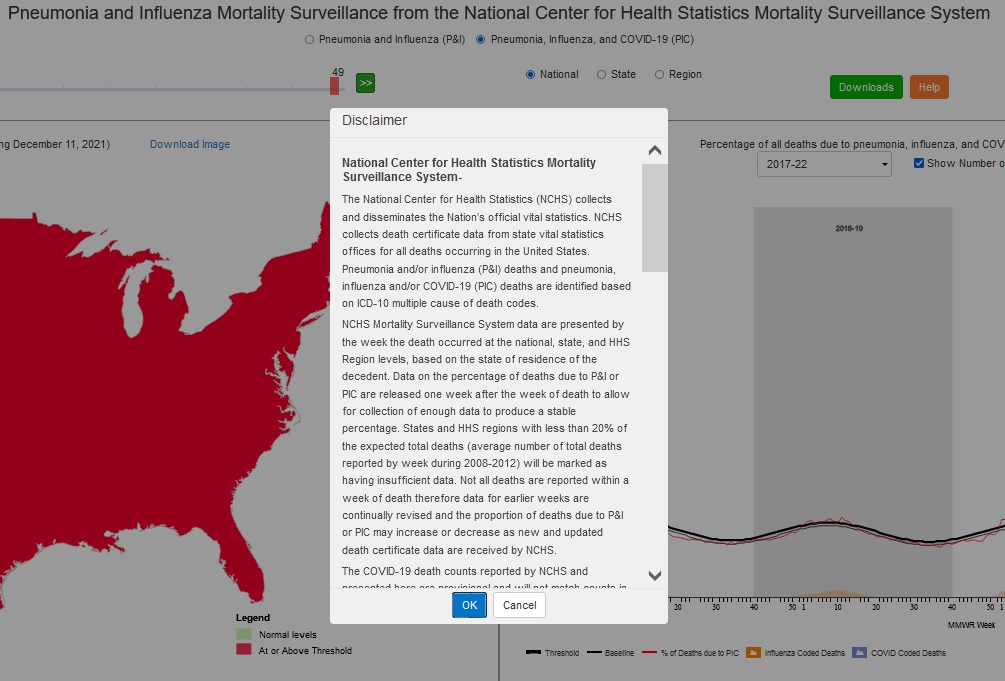
This is the legal disclaimer that appears when starting the US Centers for Disease Control (CDC’s) Fluview Interactive application which purports to report the percentage of deaths per week “due to” pneumonia and influenza (P&I) prior to March 2020 and pneumonia, influenza, and COVID-19 (PIC) since March 2020. (URL: http://gis.cdc.gov/grasp/fluview/mortality.html)
Emphasis is added to key phrases. The NOTES explain the definition and meaning of several technical terms used in the disclaimer.
The disclaimer essentially says, in plain English, the data — the COVID-19 death counts — which is presented with no estimates of statistical or systematic errors is provisional and could be entirely wrong. Two sentences in one paragraph appear to contradict one another.
National Center for Health Statistics Mortality Surveillance System-
NOTE: The National Center for Health Statistics (NCHS) is a division of the US Centers for Disease Control and Prevention (CDC).
The National Center for Health Statistics (NCHS) collects and disseminates the Nation’s official vital statistics. NCHS collects death certificate data from state vital statistics offices for all deaths occurring in the United States. Pneumonia and/or influenza (P&I) deaths and pneumonia, influenza and/or COVID-19 (PIC) deaths are identified based on ICD-10 multiple cause of death codes.
NOTE: ICD-10 is the International Classification of Diseases 10th Edition, a medical classification list by the World Health Organization (WHO). “ICD-10 multiple cause of death codes” refers to multiple “causes of death” listed on death certificates. Many death certificates have many causes of death such as emphysema, a degenerative eventually terminal condition, and pneumonia. One cause of the death is singled out as the “underlying cause of death” or UCOD. One cause of death is singled out as the “immediate cause of death.” The immediate cause of death is often not the underlying cause of death. For example, emphysema may be the underlying cause of death and pneumonia, the influenza virus, or the “common cold” may be the immediate cause of death.
NCHS Mortality Surveillance System data are presented by the week the death occurred at the national, state, and HHS Region levels, based on the state of residence of the decedent. Data on the percentage of deaths due to P&I or PIC are released one week after the week of death to allow for collection of enough data to produce a stable percentage. States and HHS regions with less than 20% of the expected total deaths (average number of total deaths reported by week during 2008-2012) will be marked as having insufficient data. Not all deaths are reported within a week of death therefore data for earlier weeks are continually revised and the proportion of deaths due to P&I or PIC may increase or decrease as new and updated death certificate data are received by NCHS.
NOTE: Notice the conflictbetween “to allow for collection of enough data to produce a stable percentage” and “the proportion of deaths due to P&I or PIC may increase or decrease as new and updated death certificate data are received by NCHS.” Percentage is a way of expressing the proportion: for example, fifty percent (a percentage) versus one half (another way of expressing the same percentage). “Stable” usually means “not changing or fluctuating” (Merriam Webster) when used in this way.
The COVID-19 death counts reported by NCHS and presented here are provisional and will not match counts in other sources, such as media reports or numbers from county health departments. COVID-19 deaths may be classified or defined differently in various reporting and surveillance systems. Death counts reported by NCHS include deaths that have COVID-19 listed as a cause of death and may include laboratory confirmed COVID-19 deaths and clinically confirmed COVID-19 deaths. Provisional death counts reported by NCHS track approximately 1-2 weeks behind other published data sources on the number of COVID-19 deaths in the U.S. These reasons may partly account for differences between NCHS reported death counts and death counts reported in other sources.
NOTE: The language “a cause of death” likely means that COVID-19 (or pneumonia or influenza in pre-2020 figures) is one of the causes of death listed on the death certificate, not necessarily the underlying cause of death (UCOD). Remember, many death certificates have multiple causes of death, one of which is identified as the underlying cause of death. (UCOD). Note also that the disclaimer specifically states that NCHS numbers “will not match..numbers from county health departments.” County health departments are presumably official, primary sources of death data with qualified staff — medical examiners and others.
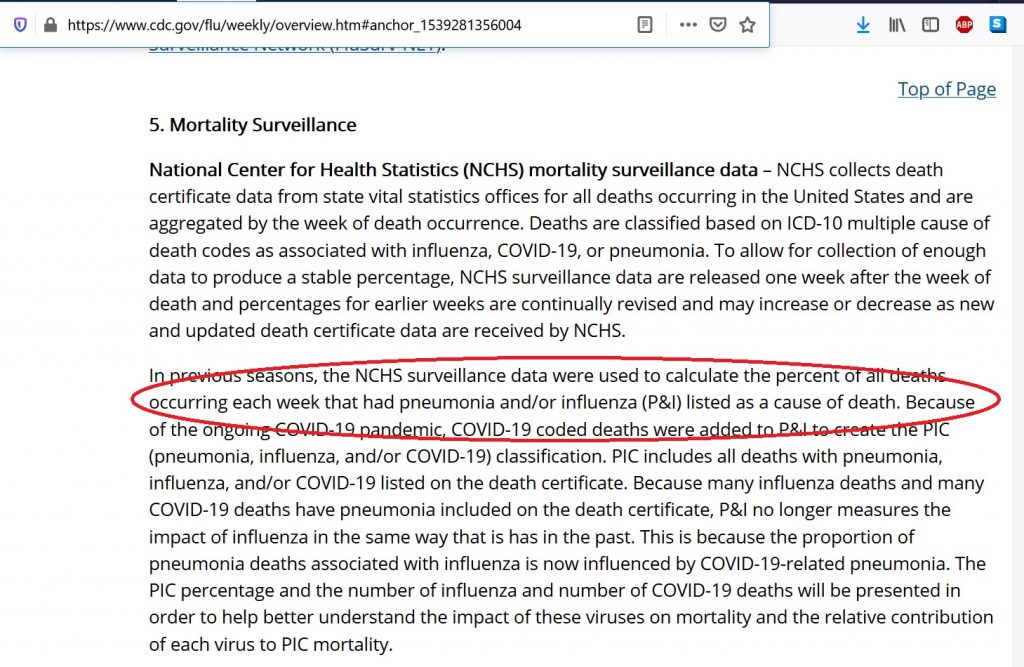
In previous seasons, the NCHS surveillance data were used to calculate the percent of all deaths occurring each week that had pneumonia and/or influenza (P&I) listed as a cause of death. Because of the ongoing COVID-19 pandemic, COVID-19 coded deaths were added to P&I to create the PIC (pneumonia, influenza, and/or COVID-19) classification. PIC includes all deaths with pneumonia, influenza, and/or COVID-19 listed on the death certificate. Because many influenza deaths and many COVID-19 deaths have pneumonia included on the death certificate, P&I no longer measures the impact of influenza in the same way that it has in the past. This is because the proportion of pneumonia deaths associated with influenza is now influenced by COVID-19-related pneumonia. The PIC percentage and the number of influenza and number of COVID-19 deaths will be presented in order to help better understand the impact of these viruses on mortality and the relative contribution of each virus to PIC mortality.
The PIC percentages are compared to a seasonal baseline of P&I deaths that is calculated using a periodic regression model that incorporates a robust regression procedure applied to data from the previous five years. An increase of 1.645 standard deviations above the seasonal baseline of P&I deaths is considered the “epidemic threshold,” i.e., the point at which the observed proportion of deaths is significantly higher than would be expected at that time of the year in the absence of substantial influenza, and now COVID-related mortality. Baselines and thresholds are calculated at the national and regional level and by age groups.
* The 10 U.S. Department of Health and Human Services regions include the following jurisdictions. Region 1: Connecticut, Main, Massachusetts, New Hampshire, Rhode Island, and Vermont; Region 2: New Jersey, New York, and New York City; Region 3: Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, and West Virginia; Region 4: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee; Region 5: Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin; Region 6: Arkansas, Louisiana, New Mexico, Oklahoma, and Texas; Region 7: Iowa, Kansas, Missouri, and Nebraska; Region 8: Colorado, Montana, North Dakota, South Dakota, Utah, and Wyoming; Region 9: Arizona, California, Hawaii, and Nevada; Region 10: Alaska, Idaho, Oregon, and Washington.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Antibody Dependent Enhancement (ADE) is a phenomenon that has been observed with a number of vaccines in which the vaccine initially produces no or negligible adverse effects but when the vaccinated person or animal actually encounters the virus or bacteria the vaccine is intended to stop, the immune system overreacts to the infection and harms or kills the vaccinated person. Prior to the COVID-19 pandemic, previous attempts to develop vaccines to prevent coronavirus infections such as SARS (2003, not SARS-COV-2) and MERS failed due to ADE.
How likely is potentially fatal antibody dependent enhancement (ADE) with the COVID-19 vaccines? Simple answer: we don’t know.We are conducting a gigantic uncontrolled experiment on a large fraction of the human race.
The Moderna clinical trials of their RNA COVID-19 vaccine, linked and discussed at the end of this article, suggest that ADE reactions in generally healthy persons similar to the test subjects in their trial are probably (95% confidence level) less than one in sixty-six (66) persons (1.5 percent) using the rule of three in statistics. This is based on a tiny sample of only 196 persons in the trial who actually developed COVID-19 — were actually exposed to the virus. ADE does not appear to have been reported in any of these 196 cases.
UPDATE (April 27, 2021): It is a bit unclear what number — 196, 11, or 185 — to use in the rule of three. The Moderna trial reported only eleven (11) vaccinated subjects with COVID-19 and 185 unvaccinated subjects with COVID-19. Thus, one could use the eleven in which case the rule of three would imply that the risk of ADE is probably less than one in 3.6. However, about 185 vaccinated subjects were exposed to COVID-19 in the vaccinated group as in the un-vaccinated control group. The vaccine worked for all but 11 of these. This would make the correct number 185 instead of 196 and give an estimate that the risk of ADE is probably (95% confidence level) less than one in sixty-one (1:61) or 1.6 percent. Most likely the correct number is about 185 (not the naive 196); the estimated bound on the risk is just about the same for 185 and 196.
References on Historical Failures of Coronavirus Vaccines due to ADE
VIII.For a vaccine to work, our immune system needs to be stimulated to produce a neutralizing antibody, as opposed to a non-neutralizing antibody. A neutralizing antibody is one that can recognize and bind to some region (‘epitope’) of the virus, and that subsequently results in the virus either not entering or replicating in your cells. A non-neutralizing antibody is one that can bind to the virus, but for some reason, the antibody fails to neutralize the infectivity of the virus. In some viruses, if a person harbors a non-neutralizing antibody to the virus, a subsequent infection by the virus can cause that person to elicit a more severe reaction to the virus due to the presence of the non-neutralizing antibody. This is not true for all viruses, only particular ones. This is called Antibody Dependent Enhancement (ADE), and is a common problem with Dengue Virus, Ebola Virus, HIV, RSV, and the family of coronaviruses. In fact, this problem of ADE is a major reason why many previous vaccine trials for other coronaviruses failed. Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place. This can cause a hyperinflammatory response, a cytokine storm, and a generally dysregulation of the immune system that allows the virus to cause more damage to our lungs and other organs of our body. In addition, new cell types throughout our body are now susceptible to viral infection due to the additional viral entry pathway. There are many studies that demonstrate that ADE is a persistent problem with coronaviruses in general, and in particular, with SARS-related viruses. ADE has proven to be a serious challenge with coronavirus vaccines, and this is the primary reason many of such vaccines have failed in early in-vitro or animal trials. For example, rhesus macaques who were vaccinated with the Spike protein of the SARS-CoV virus demonstrated severe acute lung injury when challenged with SARS-CoV, while monkeys who were not vaccinated did not. Similarly, mice who were immunized with one of four different SARS-CoV vaccines showed histopathological changes in the lungs with eosinophil infiltration after being challenged with… (EMPHASIS ADDED)
Specific references for failures of coronavirus vaccines for SARS (2003, not SARS-COV-2) and MERS are given after the following section on ADE and COVID-19/SARS-COV-2
This is a March 12, 2018 article from Children’s Health Defense (Robert F. Kennedy Jr’s group) with an overview of several cases of known or suspected antibody dependent enhancement in some vaccines with scientific references. Does not appear to discuss the coronavirus vaccine failures with ADE.
NOTE: many articles that turn up in searches now appear to omit or not clearly state that previous attempts to develop coronavirus vaccines failed due to ADE in early trials.
Abstract: Antibody-dependent enhancement (ADE) exists in several kinds of virus. It has a negative influence on antibody therapy for viral infection. This effect was first identified in dengue virus and has since also been described for coronavirus. To date, the rapid spread of the newly emerged coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing coronavirus disease 2019 (COVID-19), has affected over 3.8 million people across the globe. The novel coronavirus poses a great challenge and has caused a wave of panic. In this review, antibody-dependent enhancements in dengue virus and two kinds of coronavirus are summarized. Possible solutions for the effects are reported. We also speculate that ADE may exist in SARS-CoV-2.
Keywords: Antibody-dependent enhancement (ADE); Coronavirus disease 2019 (COVID-19); Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); Severe acute respiratory syndrome coronavirus (SARS-CoV); Middle East respiratory syndrome coronavirus (MERS-CoV)
Highlights
Five mechanisms of antibody-dependent enhancement have been discussed to date, with the most frequent effect being related to FcγR.
Antibody-dependent enhancement has been discovered in both severe acute respiratory syndrome coronavirus and Middle East respiratory syndrome coronavirus, but the mechanism is not completely clear; different studies have led to different opinions.
Many scientist have mentioned the potential existence of antibody-dependent enhancement in the 2019 novel coronavirus – severe acute respiratory syndrome coronavirus.
The most recent studies on both convalescent plasma transmission and the application of inactivated vaccine did not report any case of antibody-dependent enhancement.
Yip MS, Leung NH, Cheung CY, et al. Antibody-dependent infection of human macrophages by severe acute respiratory syndrome coronavirus. Virol J. 2014;11:82. Published 2014 May 6. doi:10.1186/1743-422X-11-82 (PDF attached to this email)
Abstract
Background
Public health risks associated to infection by human coronaviruses remain considerable and vaccination is a key option for preventing the resurgence of severe acute respiratory syndrome coronavirus (SARS-CoV). We have previously reported that antibodies elicited by a SARS-CoV vaccine candidate based on recombinant, full-length SARS-CoV Spike-protein trimers, trigger infection of immune cell lines. These observations prompted us to investigate the molecular mechanisms and responses to antibody-mediated infection in human macrophages.
Methods
We have used primary human immune cells to evaluate their susceptibility to infection by SARS-CoV in the presence of anti-Spike antibodies. Fluorescence microscopy and real-time quantitative reverse transcriptase polymerase chain reaction (RT-PCR) were utilized to assess occurrence and consequences of infection. To gain insight into the underlying molecular mechanism, we performed mutational analysis with a series of truncated and chimeric constructs of fragment crystallizable γ receptors (FcγR), which bind antibody-coated pathogens.
Results
We show here that anti-Spike immune serum increased infection of human monocyte-derived macrophages by replication-competent SARS-CoV as well as Spike-pseudotyped lentiviral particles (SARS-CoVpp). Macrophages infected with SARS-CoV, however, did not support productive replication of the virus. Purified anti-viral IgGs, but not other soluble factor(s) from heat-inactivated mouse immune serum, were sufficient to enhance infection. Antibody-mediated infection was dependent on signaling-competent members of the human FcγRII family, which were shown to confer susceptibility to otherwise naïve ST486 cells, as binding of immune complexes to cell surface FcγRII was necessary but not sufficient to trigger antibody-dependent enhancement (ADE) of infection. Furthermore, only FcγRII with intact cytoplasmic signaling domains were competent to sustain ADE of SARS-CoVpp infection, thus providing additional information on the role of downstream signaling by FcγRII.
Conclusions
These results demonstrate that human macrophages can be infected by SARS-CoV as a result of IgG-mediated ADE and indicate that this infection route requires signaling pathways activated downstream of binding to FcγRII receptors.
Liu L, Wei Q, Lin Q, et al. Anti-spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection.JCI Insight. 2019;4(4):e123158. Published 2019 Feb 21. doi:10.1172/jci.insight.123158 (PDF too large to attach to email, available on web site linked above).
Abstract
Newly emerging viruses, such as severe acute respiratory syndrome coronavirus (SARS-CoV), Middle Eastern respiratory syndrome CoVs (MERS-CoV), and H7N9, cause fatal acute lung injury (ALI) by driving hypercytokinemia and aggressive inflammation through mechanisms that remain elusive. In SARS-CoV/macaque models, we determined that anti–spike IgG (S-IgG), in productively infected lungs, causes severe ALI by skewing inflammation-resolving response. Alveolar macrophages underwent functional polarization in acutely infected macaques, demonstrating simultaneously both proinflammatory and wound-healing characteristics. The presence of S-IgG prior to viral clearance, however, abrogated wound-healing responses and promoted MCP1 and IL-8 production and proinflammatory monocyte/macrophage recruitment and accumulation. Critically, patients who eventually died of SARS (hereafter referred to as deceased patients) displayed similarly accumulated pulmonary proinflammatory, absence of wound-healing macrophages, and faster neutralizing antibody responses. Their sera enhanced SARS-CoV–induced MCP1 and IL-8 production by human monocyte–derived wound-healing macrophages, whereas blockade of FcγR reduced such effects. Our findings reveal a mechanism responsible for virus-mediated ALI, define a pathological consequence of viral specific antibody response, and provide a potential target for treatment of SARS-CoV or other virus-mediated lung injury.
Keywords: Infectious disease, Pulmonology
Keywords: Cytokines, Immunoglobulins, Macrophages
ADE in Ferrets with SARS (2003, not SARS-COV-2)
NOTE: Ferrets have a similar respiratory system to humans and are often used for animal studies of vaccines for respiratory illnesses for this reason.
Weingartl H, Czub M, Czub S, et al. Immunization with modified vaccinia virus Ankara-based recombinant vaccine against severe acute respiratory syndrome is associated with enhanced hepatitis in ferrets. J Virol. 2004;78(22):12672-12676. doi:10.1128/JVI.78.22.12672-12676.2004
Abstract
Severe acute respiratory syndrome (SARS) caused by a newly identified coronavirus (SARS-CoV) is a serious emerging human infectious disease. In this report, we immunized ferrets (Mustela putorius furo) with recombinant modified vaccinia virus Ankara (rMVA) expressing the SARS-CoV spike (S) protein. Immunized ferrets developed a more rapid and vigorous neutralizing antibody response than control animals after challenge with SARS-CoV; however, they also exhibited strong inflammatory responses in liver tissue. Inflammation in control animals exposed to SARS-CoV was relatively mild. Thus, our data suggest that vaccination with rMVA expressing SARS-CoV S protein is associated with enhanced hepatitis.
Deming D, Sheahan T, Heise M, Yount B, Davis N, et al. (2006) Vaccine Efficacy in Senescent Mice Challenged with Recombinant SARS-CoV Bearing Epidemic and Zoonotic Spike Variants . PLOS Medicine 3(12): e525. https://doi.org/10.1371/journal.pmed.0030525
In 2003, severe acute respiratory syndrome coronavirus (SARS-CoV) was identified as the etiological agent of severe acute respiratory syndrome, a disease characterized by severe pneumonia that sometimes results in death. SARS-CoV is a zoonotic virus that crossed the species barrier, most likely originating from bats or from other species including civets, raccoon dogs, domestic cats, swine, and rodents. A SARS-CoV vaccine should confer long-term protection, especially in vulnerable senescent populations, against both the 2003 epidemic strains and zoonotic strains that may yet emerge from animal reservoirs. We report the comprehensive investigation of SARS vaccine efficacy in young and senescent mice following homologous and heterologous challenge.
Methods and Findings
Using Venezuelan equine encephalitis virus replicon particles (VRP) expressing the 2003 epidemic Urbani SARS-CoV strain spike (S) glycoprotein (VRP-S) or the nucleocapsid (N) protein from the same strain (VRP-N), we demonstrate that VRP-S, but not VRP-N vaccines provide complete short- and long-term protection against homologous strain challenge in young and senescent mice. To test VRP vaccine efficacy against a heterologous SARS-CoV, we used phylogenetic analyses, synthetic biology, and reverse genetics to construct a chimeric virus (icGDO3-S) encoding a synthetic S glycoprotein gene of the most genetically divergent human strain, GDO3, which clusters among the zoonotic SARS-CoV. icGD03-S replicated efficiently in human airway epithelial cells and in the lungs of young and senescent mice, and was highly resistant to neutralization with antisera directed against the Urbani strain. Although VRP-S vaccines provided complete short-term protection against heterologous icGD03-S challenge in young mice, only limited protection was seen in vaccinated senescent animals. VRP-N vaccines not only failed to protect from homologous or heterologous challenge, but resulted in enhanced immunopathology with eosinophilic infiltrates within the lungs of SARS-CoV–challenged mice. VRP-N–induced pathology presented at day 4, peaked around day 7, and persisted through day 14, and was likely mediated by cellular immune responses.
Conclusions
This study identifies gaps and challenges in vaccine design for controlling future SARS-CoV zoonosis, especially in vulnerable elderly populations. The availability of a SARS-CoV virus bearing heterologous S glycoproteins provides a robust challenge inoculum for evaluating vaccine efficacy against zoonotic strains, the most likely source of future outbreaks.
FINAL COMMENT
How likely is potentially fatal antibody dependent enhancement (ADE) with the COVID-19 vaccines? Simple answer: we don’t know. We are conducting a gigantic uncontrolled experiment on a large fraction of the human race.
These are the trial results reported by Moderna for their now widely used RNA vaccine.
The emergency use authorization for the Moderna vaccine was based on a study of 14,134 test subjects who actually received the vaccine and not the placebo. ADE requires both being vaccinated and exposure to the virus. The Moderna study did not involve deliberately exposing the roughly 28,000 test subjects (both placebo and actually vaccinated) to SARS-COV-2. Rather the study waited for natural infection of the test subjects — a tiny number:
The median length of follow up for efficacy for participants in the study was 9 weeks post Dose 2. There were 11 COVID‑19 cases in the Moderna COVID‑19 Vaccine group and 185 cases in the placebo group, with a vaccine efficacy of 94.1% (95% confidence interval of 89.3% to 96.8%).
(from Moderna web site on April 21, 2021)
The Emergency Use Authorization (not standard FDA approval which takes years) was based on a total of 196 COVID-19 cases. Presumably these 196 patients did not exhibit ADE. Test subjects in these clinical trials for vaccine approvals — or emergency use authorization in this case — are generally quite healthy and are not a representative sample of the frail elderly at most risk from COVID-19. Thus the risk of ADE in generally healthy vaccinated persons similar to the test subjects used in the Moderna clinical trial is probably (95% confidence level) less than one in sixty-six (66) persons (1.5 percent) using the rule of three in statistics.
UPDATE (April 27, 2021): It is a bit unclear what number — 196, 11, or 185 — to use in the rule of three. The Moderna trial reported only eleven (11) vaccinated subjects with COVID-19 and 185 unvaccinated subjects with COVID-19. Thus, one could use the eleven in which case the rule of three would imply that the risk of ADE is probably less than one in 3.6. However, about 185 vaccinated subjects were exposed to COVID-19 in the vaccinated group as in the un-vaccinated control group. The vaccine worked for all but 11 of these. This would make the correct number 185 instead of 196 and give an estimate that the risk of ADE is probably (95% confidence level) less than one in sixty-one (1:61) or 1.6 percent. Most likely the correct number is about 185 (not the naive 196); the estimated bound on the risk is just about the same for 185 and 196.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This article argues that the US Centers for Disease Control (CDC)’s April 2020 guidance for filling out death certificates for possible COVID-19 related deaths strongly encourages, if not requires, assigning COVID-19 as the underlying cause of death (UCOD) in any death where COVID-19 or the SARS-COV-2 virus may be present, which appears to differ from common historical practice for pneumonia and influenza deaths where pneumonia was frequently treated as a “complication,” a cause of death but not the underlying cause of death.
This means the number of COVID deaths should be compared to a count of death certificates where pneumonia and influenza were listed as a cause of death or even a lesser contributing factor, a historical number which appears to have been at least 188,000 per year based on the CDC FluView web site. The proper comparison number may be even larger if deaths that historically were listed as heart attacks, cancer or other causes than pneumonia or influenza are also being reassigned due to the April 2020 guidance.
The CDC has at least three different historical pneumonia and influenza death numbers. These are the leading causes of death report numbers of about 55,000 deaths per year which appears based on death certificates, a poorly documented mathematical/computer model which attributes about 55,000 deaths per year with a large error to the influenza virus, and the FluView web site which attributed about 188,000 deaths per year to pneumonia and influenza.
The leading causes of death historical numbers appear based on the underlying cause of death listed on the death certificate whereas the FluView historical numbers appear based on death certificates that list pneumonia or influenza as a cause of death, in most cases not the underlying cause of death. The historical FluView death numbers appear to be the proper baseline for comparison to COVID-19, although an even larger number is possible if there has been practically significant reassignment of heart attacks and other deaths as well.
This would mean that COVID-19 is less deadly than popular perceptions based frequently on comparisons to “flu death numbers” of about 55,000 per year apparently derived either from the CDC’s leading causes of death report or the influenza virus model.
Note that this is not a claim that COVID-19 or SARS-COV-2 plays no causal role in the deaths: a death “with” COVID rather than a death “due to” COVID in popular debates. Rather, the proper interpretation is probably that COVID-19 acts predominantly as an opportunistic infection instead of an inherently deadly infection able to easily kill healthy young people with a strong immune system. Vaccines are likely to have small or no ability to prevent death from an opportunistic infection since the infected vaccinated person will have a weak or failed immune system with little or no ability to produce the immune response learned from the vaccination.
The language and numbers on the CDC web sites and official reports and documents are remarkably confusing and grossly contradictory in some cases — such as the historical number of deaths attributed to pneumonia and influenza which differs by over a factor of THREE. Error bars or confidence levels on most numbers such as the death numbers are not reported as required by common scientific and engineering practice. These practices have been harshly criticized for years by scientists and medical experts such as Peter Doshi. Consequently it is impossible to make definite statements about the meaning of the numbers and the definitions of measured quantities discussed below.
This is a complex life-and-death subject with many nuances. Each section below expands each key point in detail, discussing the nuances and unknowns. Some facts and arguments are repeated in different sections for clarity.
Three Different Historical Pneumonia and Influenza Death Numbers
The United States Centers for Disease Control (CDC) documents and web site present at least THREE different historical (pre-2020) estimates of deaths from “influenza and pneumonia,” “pneumonia and influenza,” and/or “influenza” or the “flu” presumably meaning the influenza category of viruses. Which of these three death numbers, one of which differs by a factor of OVER THREE from the other two, should be compared to COVID-19 deaths? Indeed, it could well be incorrect to compare any of them to the COVID-19 deaths.
These three pneumonia and influenza death numbers are the value in the annual leading causes of death report — about 55,000 deaths each year, the tables of “pneumonia and influenza” (abbreviated as P&I) from the National Center for Health Statistics (NCSH) used on the FluView web site — about 188,000 deaths per year, OVER THREE TIMES the leading causes of death number, and the output of a poorly documented model of deaths attributed to the influenza category of viruses, a broad range centered at about 55,000 deaths per year.
Deaths attributed to COVID-19 in 2020 have frequently been compared to an estimate of about 55,000, either to the date of the report or for the entire year. The language used is often unclear but appears to refer to either the CDC’s influenza mathematical model or the leading causes of death number, which are similar numbers but technically not the same.
This article argues that the current COVID-19 death numbers are best compared to the larger FluView numbers, although an even larger different number may be appropriate if deaths that would have been attributed to heart attacks, strokes, or other blood coagulation related disorders in the absence of a positive SARS-COV-2 test or diagnosis are included in the current COVID-19 death counts.
The CDC FluView Web Site
The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluViewPneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list about 188,000 deaths per year attributed to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
Note also that deaths attributed to “pneumonia and influenza” on the FluView web site are highly seasonal. A substantial increase over the summer is expected during the winter (or rainy season in Northern California and similar regions), peaking in December and January each year.
Also note that the seasonal variation is sinusoidal — like the oscillation of a pendulum or a mechanical spring. Contrary to popular culture, there is no clear step up when schools open in the fall or step down when schools close for the summer. It looks very much like something driven by the Sun, directly or indirectly by some mechanism or mechanisms. Possible mechanisms include Vitamin D production from sunlight, destruction of viruses and bacteria in the air or on surfaces by ultraviolet light in sunlight, general health benefits of a warm environment, or some other Sun-driven phenomenon.
The Leading Causes of Death Report
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
A longer, more detailed discussion of the FluView, leading causes of death, and the CDC’s influenza virus death model death numbers (yet another number) may be found below. It appears likely the FluView death numbers are defined similarly to current COVID-19 death counts; the reasons for this are explained in some detail.
Which Pneumonia and Influenza Death Numbers Should Be Compared to the COVID-19 Death Numbers?
The FluView and Leading Causes of Death numbers for “pneumonia and influenza” differ by a factor of OVER THREE. Note that both the FluView and Leading Causes of Death numbers have no error bars or error estimates given, implying exact numbers in common scientific and engineering practice. Should the number of COVID-19 deaths be compared to the FluView number or the leading causes of death number or some other number?
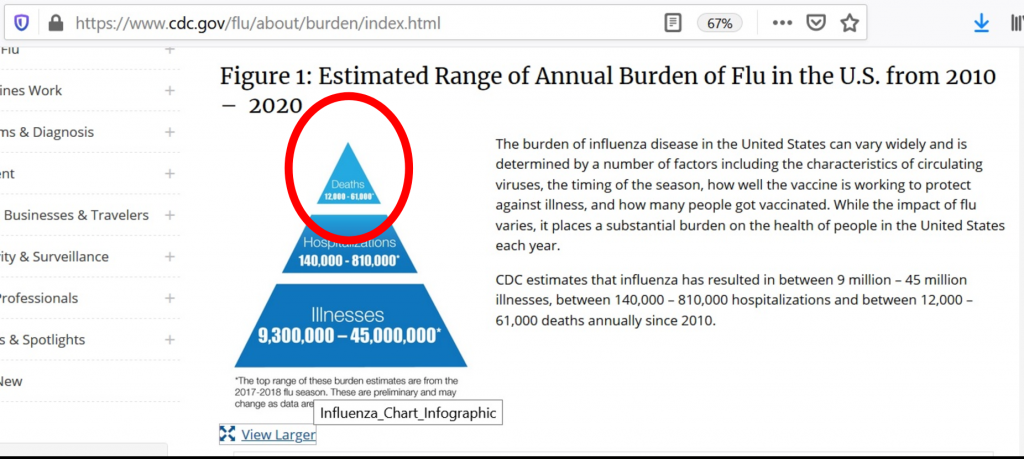
The CDC also uses a poorly documented mathematical model that attributes roughly 55,000 deaths from pneumonia and influenza to the influenza virus as the underlying cause, a number roughly comparable to the total pneumonia and influenza deaths in the leading causes of death. The influenza virus is confirmed by laboratory tests in only a small fraction of pneumonia and influenza deaths, about 6,000 per year.
Although the language is often unclear in the CDC documents and web site, the CDC appears to claim that an initial influenza infection which disappears or becomes undetectable in laboratory tests leads to the subsequent pneumonia, presumably a bacterial pneumonia although other viruses would be consistent with some lab tests. Based on this argument, the CDC appears to attribute most pneumonia deaths where historically pneumonia was listed as the “underlying cause of death” to the influenza virus for which there is a flu vaccine that the CDC promotes heavily — even though laboratory tests frequently fail to confirm influenza or even detect other viruses or bacteria instead. The “underlying cause of death” is discussed in more detail below.
As shown in the graphic above, the CDC web site Disease Burden of Influenza (Figure 1) appears to give a range from 12,000 to 61,000 influenza deaths from this model. The graphic does not indicate if this range is a 95 percent confidence interval — a common scientific and engineering practice — or some other error estimate. The range in the graphic does not appear to match any of the 95 percent confidence levels for estimated deaths attributed to influenza in Table 1.
The History of Serious Criticism of the CDC’s “Flu” Death Numbers
There is a long history of serious criticism of the CDC’s “flu” death numbers by medical scientists and others. The most prominent critic is Peter Doshi, currently a professor at the University of Maryland and an associate editor at the British Medical Journal.
Citing the results of actual laboratory tests of deceased patients, critics of the CDC’s flu death numbers such as University of Maryland Professor Peter Doshi have argued that pneumonia deaths are due to a range of different viruses, bacteria, other pathogens, and even toxins, rather than predominantly influenza as implied by the CDC’s influenza deaths model. The output of this model appears to be the basis of the baseline “flu” deaths numbers used in most popular and public policy discussions of COVID-19 deaths — although the leading causes of death report number may also be used.
The Reason for the Large Difference Between the FluView and Leading Causes of Death Numbers
The US CDC documents and web site are frequently unclear and even contradictory as in the case of these grossly contradictory totals of deaths from pneumonia and influenza. This makes it difficult to be certain of the cause for the difference. Nonetheless, the technical notes for each document — FluView and the leading causes of death — give a highly probable reason.
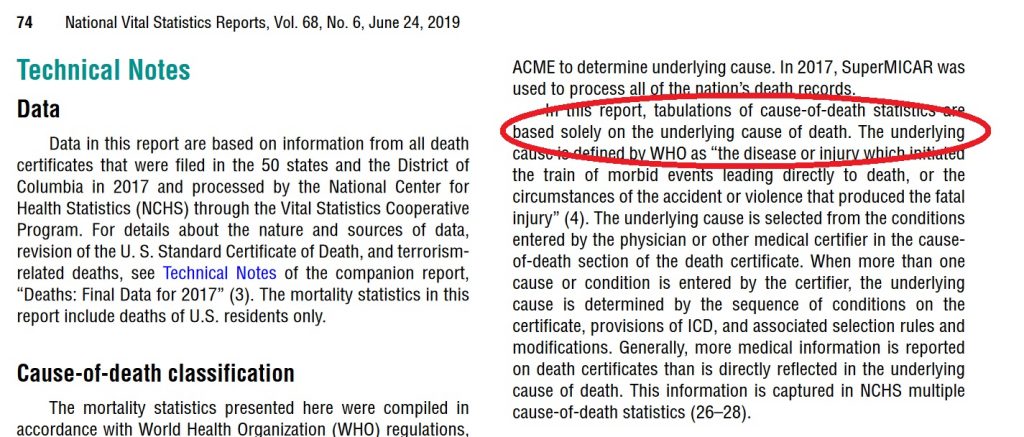
Leading Causes of Death Report for 2017 with “the underlying cause of death” language circled in red. (Dec. 18, 2020)
Death certificates frequently have multiple causes of death. One of these is assigned as the underlying cause of death. This may be quite arbitrary in some cases. Indeed the concept of “underlying cause of death” may not be well defined for some deaths because the aged may develop multiple health problems in parallel that are fatal in combination.
FluView Mortality Surveillance notes with “A Cause of Death” Language Circled in Red (Dec. 18, 2020)
The Rules for Assigning the Underlying Cause of Death Before COVID-19
Prior to 2020 and COVID-19, most pneumonia deaths did not list pneumonia or the pneumonia-causing pathogen if known as the underlying cause of death. This will be discussed in detail below. The only common partial exception was HIV/AIDS where pneumocystis carinii pneumonia (a common fungus) was often the immediate cause of death and the Human Immunodeficiency Virus (HIV) is almost always listed as the underlying cause of death. However, HIV is not the pneumonia-causing pathogen which is the pneumocystis fungus. Instead, most pneumonia deaths, those included in the FluView numbers but not included in the leading causes of death numbers, were attributed to a cause such as a chronic lower respiratory disease, heart disease, cancer, even accidents, and other usually pre-existing conditions as the underlying cause of death.
The CDC follows the World Health Organization (WHO)’s definition of the underlying cause of death. WHO defines the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury” in accordance with the rules of the International Classification of Diseases (ICD).
In the United States, the underlying cause of death is listed last in the list of causes of death in part I of the death certificate. The immediate cause of death is listed first. Part 2 lists other conditions that are considered contributing factors but somehow not causes. Pneumonia is often the immediate cause of death in part 1 of the death certificate.
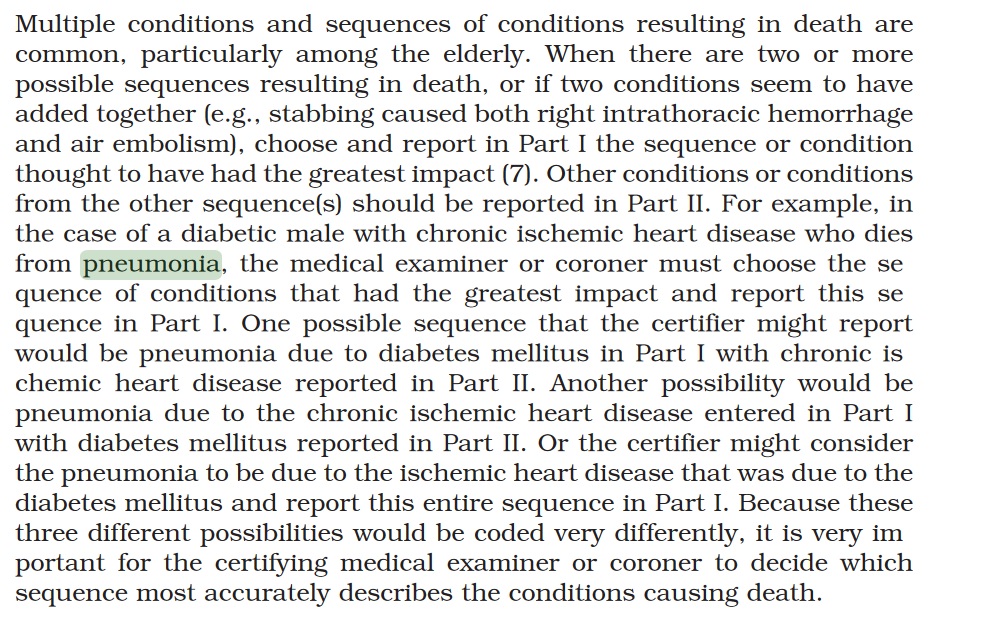
In principle, death certificates and the assignment of causes of death including the underlying cause of death is governed or at least guided by the CDC’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (2003 Revision). This one-hundred and thirty-eight (138) page manual actually provides very limited guidance on how to assign the underlying cause of death in cases where pneumonia is present. Page twenty-five (25) has the only detailed discussion of deaths involving pneumonia:
US CDC Medical Examiners’ Handbook 2003 suggests attributing a pneumonia death to either chronic ischemic heart disease or diabetes mellitus as the underlying cause but not the pneumonia or pneumonia-causingpathogen. No clear direction to the physician.
Pneumonia is often a nonspecific process that occurs as the terminal event in someone who dies of a more specific underlying cause of death, such as congestive heart failure resulting from ischemic heart disease. In such cases, the specific underlying cause of death should be included in the cause-of-death statement.
Pneumonia is often designated as either community acquired or hospital or institution acquired (nosocomial). If the community- or institution-acquired nature of the pneumonia is known, the cause-of-death statement should include an indication of which one applies.
The specific bacterial, viral, or other infectious agent, if known, should be cited in the cause-of-death statement.
Relevant risk factors should also be cited in the cause-of-death statement, as might occur in an alcoholic who develops tuberculous pneumonia. Only in those instances where pneumonia has caused death and there is no known underlying cause or risk factor should the underlying cause of death be stated as “Pneumonia,” being sure to specify the infectious agent, if known, or specifying that a specific etiology is unknown, if such is the case.
Emphasis Added
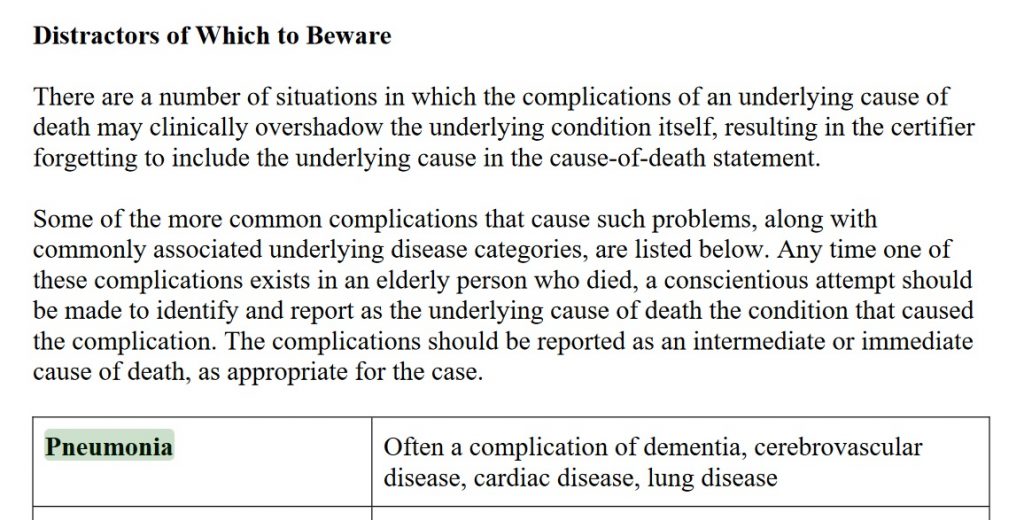
And on page 113 of Cause of Death and the Death Certificate by Randy Hanzlick, dementia, cerebrovascular disease, cardiac disease, and lung disease are all listed as common underlying causes of death in cases of deaths due to pneumonia:
Thus, traditionally, pre-2020 and COVID-19, pneumonia deaths were frequently assigned a non-pneumonia underlying cause of death, usually a pre-existing condition and not the pneumonia-causing pathogen such as the influenza virus or SARS-COV-2, in common medical practice. Based on the technical notes these pneumonia and influenza deaths would be included in the FluView death numbers but not in the leading causes of death report.
Comparing COVID-19 Death Numbers to the Pneumonia and Influenza Death Numbers and Estimates from Previous Years
As shown above, the CDC has at least three (3) different pneumonia and influenza death numbers and estimates: the Leading Causes of Death Report (about 55,000 deaths per year, about two percent of annual deaths from all causes), the FluView graph and underlying data from the NCHS (about 188,000 deaths per year, six to ten percent of annual deaths from all causes, before 2020), and the influenza death model estimates that range from 12,000 to 61,000 deaths per year with the best estimate close to the number of pneumonia and influenza deaths in the leading causes of death report. Are any of these the proper baseline for comparing COVID-19 deaths to prior years or should some other number or estimate be used?
In the absence of the RT-PCR and antibody tests for the SARS-COV-2 virus, most COVID-19 deaths would have been unexplained pneumonia deaths lacking a laboratory test confirming influenza or other known pathogen. Possibly, some COVID-19 deaths would have been listed as heart attacks or strokes, those COVID-19 deaths attributed to the blood clots and other blood-related anomalies currently blamed on COVID-19, or even some other causes. The rest of this article will focus on the pneumonia deaths which would probably comprise most of the COVID-19 deaths in the absence of laboratory tests.
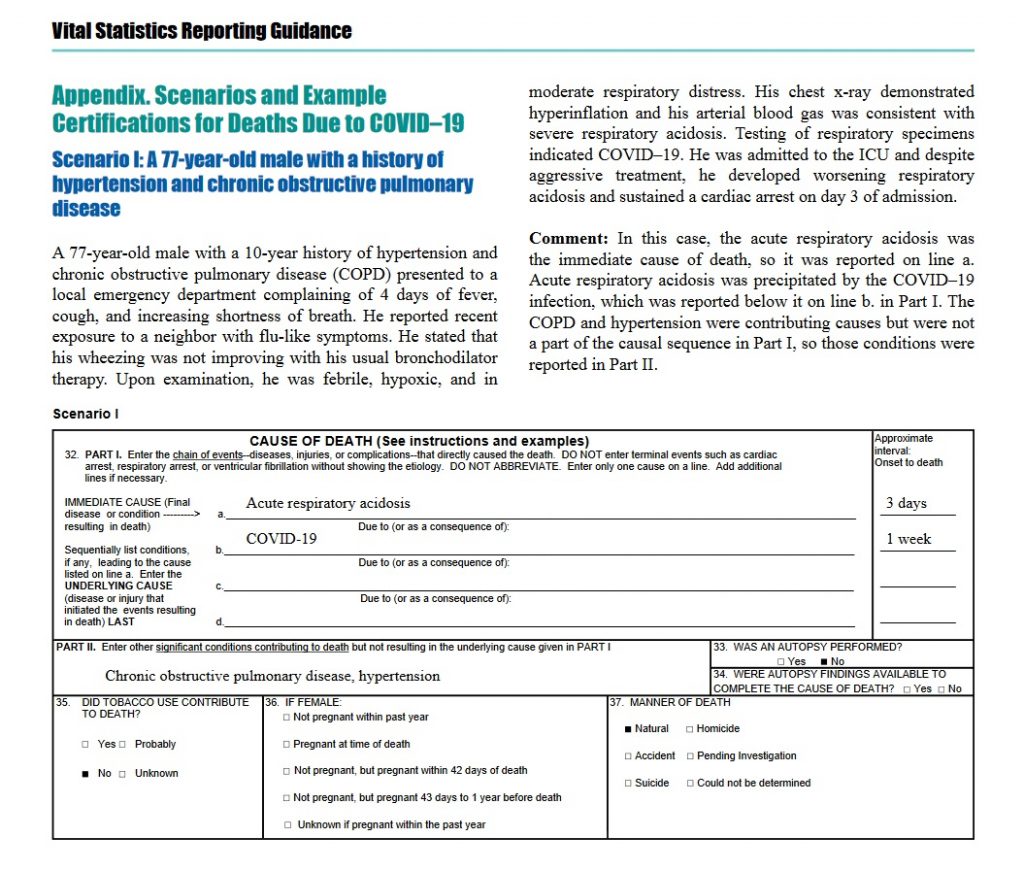
The US CDC’s April 2020 guidelines for reporting COVID-19 deaths clearly direct physicians and others not to list chronic obstructive pulmonary disease (COPD) as the underlying cause of death in COVID-19 cases, moving it to Part 2 of the death certificate reserved for “non-cause” contributing factors, which differs dramatically from medical practice prior to 2020 as described in Randy Hanzlick’s book and implicit in the FluView pneumonia and influenza deaths data.
In some cases, survival from COVID–19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID–19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II and not in Part I.
This guidance also gives a specific example of a COVID-19 death with COPD relegated to Part 2:
COVID-19 Death Guidance Example with COPD as Contributing Factor Only
Although other causes of death that are often given as the underlying cause of death in pneumonia cases on pre-2020 death certificates are not explicitly identified in the April 2020 guidance document, it seems probable most physicians would move these pre-existing conditions to Part 2 and not list them as the underlying cause of death for COVID-19 based on the April 2020 CDC guidance document. Note that COPD would fall under the category “lung disease” in the list below from Randy Hanzlick’s Causes of Death and the Death Certificate:
Thus, COVID-19 deaths since the April 2020 guidance are probably roughly comparable to the FluView deaths, the larger number, the 188,000 pneumonia and influenza deaths per year. The language “roughly” is used because the April 2020 guidance appears to strongly encourage physicians and others to assign COVID-19 as the underlying cause of death in any death where COVID-19 is detected by tests or perhaps even just suspected, raising the possibility that heart attack and stroke deaths might be wrongly classified as COVID-19 deaths as well as the traditional pneumonia and influenza deaths that would be listed in the FluView data. These would presumably be misclassified as the COVID-19 deaths exhibiting the mysterious blood clots and other blood-related problems reported in some COVID-19 cases and deaths. Thus, the FluView death numbers may represent a lower bound on COVID-19 deaths rather than an exact baseline — unfortunately.
Ealy et al have raised the question whether the CDC complied with the Paperwork Reduction Act (PRA) and Information Quality Act (IQA) requirements in issuing the April and earlier March COVID-19 death certification guidelines, apparently without submitting these for public comment through the Federal Register as Ealy and co-authors claim is required by these federal laws.
Conclusion
Thus, due to the guidance on the death certificates from the CDC in April 2020, COVID-19 deaths on death certificates appear comparable to the larger FluView death numbers — or even larger numbers if heart attacks, strokes or other blood coagulation related deaths with a positive test or clinical diagnosis are being classified as COVID-19 deaths.
The CDC’s documents and web site are remarkably unclear, contradictory, and confusing for public health and scientific information presented to the general public, busy doctors and other medical professionals, or even research scientists — as previously noted by Peter Doshi and others.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Many Seeming Routes for Efficient Spread of COVID-19 in Santa Clara County, California (USA)
Twenty minute video on many seeming routes for efficient spread of COVID-19 in Santa Clara County, California, USA (Silicon Valley). Discusses herding of residents into Big Box retail stores such as Safeway, Target, and Walmart, large apartment complexes, the VTA bus system, and construction projects with many shared spaces and surfaces.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The United States Centers for Disease Control (CDC) documents and web site present at least THREE different historical (pre-2020) estimates of deaths from “influenza and pneumonia,” “pneumonia and influenza,” and/or “influenza” or the “flu” presumably meaning the influenza category of viruses. Which of these three death numbers, one of which differs by a factor of OVER THREE from the other two, should be compared to COVID-19 deaths? Indeed, it could well be incorrect to compare any of them to the COVID-19 deaths.
These three pneumonia and influenza death numbers are the value in the annual leading causes of death report — about 55,000 deaths each year, the tables of “pneumonia and influenza” (abbreviated as P&I) from the National Center for Health Statistics (NCSH) used on the FluView web site — about 188,000 deaths per year, OVER THREE TIMES the leading causes of death number, and the output of a mysterious model of deaths attributed to the influenza category of viruses, a broad range centered at about 55,000 deaths per year.
Deaths attributed to COVID-19 in 2020 have frequently been compared to an estimate of about 55,000, either to the date of the report or for the entire year. The language used is often unclear but appears to refer to either the CDC’s influenza mathematical model or the leading causes of death number, which are similar numbers but technically not the same.
This article argues that the current COVID-19 death numbers are best compared to the larger FluView numbers, although an even larger different number may be appropriate if deaths that would have been attributed to heart attacks, strokes, or other blood coagulation related disorders in the absence of a positive SARS-COV-2 test or diagnosis are included in the current COVID-19 death counts.
The CDC FluView Web Site
The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluView Pneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list about 188,000 deaths per year attributed to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
Note also that deaths attributed to “pneumonia and influenza” on the FluView web site are highly seasonal. A substantial increase over the summer is expected during the winter (or rainy season in Northern California and similar regions), peaking in December and January each year.
Also note that the seasonal variation is sinusoidal — like the oscillation of a pendulum or a mechanical spring. Contrary to popular culture, there is no clear step up when schools open in the fall or step down when schools close for the summer. It looks very much like something driven by the Sun, directly or indirectly by some mechanism or mechanisms. Possible mechanisms include Vitamin D production from sunlight, destruction of viruses and bacteria in the air or on surfaces by ultraviolet light in sunlight, general health benefits of a warm environment, or some other Sun-driven phenomenon.
The Leading Causes of Death Report
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
A longer, more detailed discussion of the FluView, leading causes of death, and the CDC’s influenza virus death model death numbers (yet another number) may be found below. It appears likely the FluView death numbers are defined similarly to current COVID-19 death counts; the reasons for this are explained in some detail.
US CDC Leading Causes of Death Report Attributes Only About Two Percent of All Deaths to Pneumonia and Influenza (Line Item 8: Influenza and Pneumonia) — not the Six to Ten Percent in the FluView Graphs
Which Pneumonia and Influenza Death Numbers Should Be Compared to the COVID-19 Death Numbers?
The FluView and Leading Causes of Death numbers for “pneumonia and influenza” differ by a factor of OVER THREE. Note that both the FluView and Leading Causes of Death numbers have no error bars or error estimates given, implying exact numbers in common scientific and engineering practice. Should the number of COVID-19 deaths be compared to the FluView number or the leading causes of death number or some other number?
The CDC also uses a mysterious mathematical model that attributes roughly 55,000 deaths from pneumonia and influenza to the influenza virus as the underlying cause, a number roughly comparable to the total pneumonia and influenza deaths in the leading causes of death. The influenza virus is confirmed by laboratory tests in only a small fraction of pneumonia and influenza deaths, about 6,000 per year.
Although the language is often unclear in the CDC documents and web site, the CDC appears to claim that an initial influenza infection which disappears or becomes undetectable in laboratory tests leads to the subsequent pneumonia, presumably a bacterial pneumonia although other viruses would be consistent with some lab tests. Based on this argument, the CDC appears to attribute most pneumonia deaths where historically pneumonia was listed as the “underlying cause of death” to the influenza virus for which there is a flu vaccine that the CDC promotes heavily — even though laboratory tests frequently fail to confirm influenza or even detect other viruses or bacteria instead. The “underlying cause of death” is discussed in more detail below.
As shown in the graphic above, the CDC web site Disease Burden of Influenza (Figure 1) appears to give a range from 12,000 to 61,000 influenza deaths from this model. The graphic does not indicate if this range is a 95 percent confidence interval — a common scientific and engineering practice — or some other error estimate. The range in the graphic does not appear to match any of the 95 percent confidence levels for estimated deaths attributed to influenza in Table 1.
The History of Serious Criticism of the CDC’s “Flu” Death Numbers
There is a long history of serious criticism of the CDC’s “flu” death numbers by medical scientists and others. The most prominent critic is Peter Doshi, currently a professor at the University of Maryland and an associate editor at the British Medical Journal.
Citing the results of actual laboratory tests of deceased patients, critics of the CDC’s flu death numbers such as University of Maryland Professor Peter Doshi have argued that pneumonia deaths are due to a range of different viruses, bacteria, other pathogens, and even toxins, rather than predominantly influenza as implied by the CDC’s influenza deaths model. The output of this model appears to be the basis of the baseline “flu” deaths numbers used in most popular and public policy discussions of COVID-19 deaths — although the leading causes of death report number may also be used.
Why the Large Difference Between the FluView and Leading Causes of Death Numbers
The US CDC documents and web site are frequently unclear and even contradictory as in the case of these grossly contradictory totals of deaths from pneumonia and influenza. This makes it difficult to be certain of the cause for the difference. Nonetheless, the technical notes for each document — FluView and the leading causes of death — give a highly probable reason.
Leading Causes of Death Report for 2017 with “the underlying cause of death” language circled in red. (Dec. 18, 2020)
Death certificates frequently have multiple causes of death. One of these is assigned as the underlying cause of death. This may be quite arbitrary in some cases. Indeed the concept of “underlying cause of death” may not be well defined for some deaths because the aged may develop multiple health problems in parallel that are fatal in combination.
In contrast, the FluView site, the much larger number of deaths, appears to count deaths where pneumonia or influenza is listed as “a cause of death,” even if it is not the “underlying cause of death.”
FluView Mortality Surveillance notes with “A Cause of Death” Language Circled in Red (Dec. 18, 2020)
The Rules for Assigning the Underlying Cause of Death Before COVID-19
Prior to 2020 and COVID-19, most pneumonia deaths did not list pneumonia or the pneumonia-causing pathogen if known as the underlying cause of death. This will be discussed in detail below. The only common partial exception was HIV/AIDS where pneumocystis carinii pneumonia (a common fungus) was often the immediate cause of death and the Human Immunodeficiency Virus (HIV) is almost always listed as the underlying cause of death. However, HIV is not the pneumonia-causing pathogen which is the pneumocystis fungus. Instead, most pneumonia deaths, those included in the FluView numbers but not included in the leading causes of death numbers, were attributed to a cause such as a chronic lower respiratory disease, heart disease, cancer, even accidents, and other usually pre-existing conditions as the underlying cause of death.
The CDC follows the World Health Organization (WHO)’s definition of the underlying cause of death. WHO defines the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury” in accordance with the rules of the International Classification of Diseases (ICD).
In the United States, the underlying cause of death is listed last in the list of causes of death in part I of the death certificate. The immediate cause of death is listed first. Part 2 lists other conditions that are considered contributing factors but somehow not causes. Pneumonia is often the immediate cause of death in part 1 of the death certificate.
In principle, death certificates and the assignment of causes of death including the underlying cause of death is governed or at least guided by the CDC’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (2003 Revision). This one-hundred and thirty-eight (138) page manual actually provides very limited guidance on how to assign the underlying cause of death in cases where pneumonia is present. Page twenty-five (25) has the only detailed discussion of deaths involving pneumonia:
US CDC Medical Examiners’ Handbook 2003 suggests attributing a pneumonia death to either chronic ischemic heart disease or diabetes mellitus as the underlying cause but not the pneumonia or pneumonia-causingpathogen. No clear direction to the physician.
Pneumonia is often a nonspecific process that occurs as the terminal event in someone who dies of a more specific underlying cause of death, such as congestive heart failure resulting from ischemic heart disease. In such cases, the specific underlying cause of death should be included in the cause-of-death statement.
Pneumonia is often designated as either community acquired or hospital or institution acquired (nosocomial). If the community- or institution-acquired nature of the pneumonia is known, the cause-of-death statement should include an indication of which one applies.
The specific bacterial, viral, or other infectious agent, if known, should be cited in the cause-of-death statement.
Relevant risk factors should also be cited in the cause-of-death statement, as might occur in an alcoholic who develops tuberculous pneumonia. Only in those instances where pneumonia has caused death and there is no known underlying cause or risk factor should the underlying cause of death be stated as “Pneumonia,” being sure to specify the infectious agent, if known, or specifying that a specific etiology is unknown, if such is the case.
Emphasis Added
And on page 113 of Cause of Death and the Death Certificate by Randy Hanzlick, dementia, cerebrovascular disease, cardiac disease, and lung disease are all listed as common underlying causes of death in cases of deaths due to pneumonia:
Thus, traditionally, pre-2020 and COVID-19, pneumonia deaths were frequently assigned a non-pneumonia underlying cause of death, usually a pre-existing condition and not the pneumonia-causing pathogen such as the influenza virus or SARS-COV-2, in common medical practice. Based on the technical notes these pneumonia and influenza deaths would be included in the FluView death numbers but not in the leading causes of death report.
Comparing COVID-19 Death Numbers to the Pneumonia and Influenza Death Numbers and Estimates from Previous Years
As shown above, the CDC has at least three (3) different pneumonia and influenza death numbers and estimates: the Leading Causes of Death Report (about 55,000 deaths per year, about two percent of annual deaths from all causes), the FluView graph and underlying data from the NCHS (about 188,000 deaths per year, six to ten percent of annual deaths from all causes, before 2020), and the influenza death model estimates that range from 12,000 to 61,000 deaths per year with the best estimate close to the number of pneumonia and influenza deaths in the leading causes of death report. Are any of these the proper baseline for comparing COVID-19 deaths to prior years or should some other number or estimate be used?
In the absence of the RT-PCR and antibody tests for the SARS-COV-2 virus, most COVID-19 deaths would have been unexplained pneumonia deaths lacking a laboratory test confirming influenza or other known pathogen. Possibly, some COVID-19 deaths would have been listed as heart attacks or strokes, those COVID-19 deaths attributed to the blood clots and other blood-related anomalies currently blamed on COVID-19, or even some other causes. The rest of this article will focus on the pneumonia deaths which would probably comprise most of the COVID-19 deaths in the absence of laboratory tests.
The US CDC’s April 2020 guidelines for reporting COVID-19 deaths clearly direct physicians and others not to list chronic obstructive pulmonary disease (COPD) as the underlying cause of death in COVID-19 cases, moving it to Part 2 of the death certificate reserved for “non-cause” contributing factors, which differs dramatically from medical practice prior to 2020 as described in Randy Hanzlick’s book and implicit in the FluView pneumonia and influenza deaths data.
In some cases, survival from COVID–19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID–19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II and not in Part I.
This guidance also gives a specific example of a COVID-19 death with COPD relegated to Part 2:
COVID-19 Death Guidance Example with COPD as Contributing Factor Only
Although other causes of death that are often given as the underlying cause of death in pneumonia cases on pre-2020 death certificates are not explicitly identified in the April 2020 guidance document, it seems probable most physicians would move these pre-existing conditions to Part 2 and not list them as the underlying cause of death for COVID-19 based on the April 2020 CDC guidance document. Note that COPD would fall under the category “lung disease” in the list below from Randy Hanzlick’s Causes of Death and the Death Certificate:
Thus, COVID-19 deaths since the April 2020 guidance are probably roughly comparable to the FluView deaths, the larger number, the 188,000 pneumonia and influenza deaths per year. The language “roughly” is used because the April 2020 guidance appears to strongly encourage physicians and others to assign COVID-19 as the underlying cause of death in any death where COVID-19 is detected by tests or perhaps even just suspected, raising the possibility that heart attack and stroke deaths might be wrongly classified as COVID-19 deaths as well as the traditional pneumonia and influenza deaths that would be listed in the FluView data. These would presumably be misclassified as the COVID-19 deaths exhibiting the mysterious blood clots and other blood-related problems reported in some COVID-19 cases and deaths. Thus, the FluView death numbers may represent a lower bound on COVID-19 deaths rather than an exact baseline — unfortunately.
Ealy et al have raised the question whether the CDC complied with the Paperwork Reduction Act (PRA) and Information Quality Act (IQA) requirements in issuing the April and earlier March COVID-19 death certification guidelines, apparently without submitting these for public comment through the Federal Register as Ealy and co-authors claim is required by these federal laws.
Conclusion
Thus, due to the guidance on the death certificates from the CDC in April 2020, COVID-19 deaths on death certificates appear comparable to the larger FluView death numbers — or even larger numbers if heart attacks, strokes or other blood coagulation related deaths with a positive test or clinical diagnosis are being classified as COVID-19 deaths.
The CDC’s documents and web site are remarkably unclear, contradictory, and confusing for public health and scientific information presented to the general public, busy doctors and other medical professionals, or even research scientists — as previously noted by Peter Doshi and others.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
In spite of and even because of the stay-at-home, lockdown and other restrictions by health authorities in Santa Clara County, California (USA), there are many plausible routes for rapid efficient spread of the SARS-COV-2 virus presumed to cause COVID-19 in the county. Despite this, total deaths attributed to COVID-19 in the year 2020 remained remarkably low, comparable to expected deaths from pneumonia and influenza in prior years. This may of course change in the coming year.
Many probable routes of transmission are discussed and illustrated with pictures below.
Many Seeming Routes for Rapid Spread of the Disease
Santa Clara County, California (United States) continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May. The lockdown herds large numbers of citizens into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease. The lockdown also confines a large proportion of residents to large apartment complexes with many seemingly easy routes of transmission. “Essential” workers and others continue to use the county bus service which confines workers and others to an enclosed shared space for many minutes each day.
Ongoing Construction Projects
Santa Clara County continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May — several weeks after the original lockdown order. On a personal note, a four-story luxury apartment building construction project with at least a dozen workers every weekday from about 7:30 am to 4:30 pm has continued across the street from my apartment building since the original lockdown order except for the brief shutdown in May.
Santa Clara County Allows Construction Projects Despite COVID-19Over a Dozen Construction Workers Arriving for Work on Luxury Apartment Project in Santa Clara County, CA (August 6, 2020)Construction Workers in Close Proximity (Santa Clara County, Dec. 7, 2020)
Herding Residents into Big Box Retail Stores
The lockdown continues to herd large numbers of citizens in Santa Clara County into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease.
Safeway with Over Thirty Cars in Parking Lot (about 9:30 AM, December 7, 2020, Santa Clara County)
These giant “Big Box” retail stores have heavily used shared spaces and surfaces where one would expect the virus will rapidly spread. These include the entry/exit door areas, checkout counters, and refrigerators with popular products such as milk purchased by a large fraction of the customers and with door handlesthat all purchasers must use. These large stores often have hundreds of patrons in the store at the same time — all day, seven days per week.
Milk and other dairy products in a refrigerator with door handle that customers must use
In Santa Clara County, the lockdowns have closed or heavily curtailed restaurants, popular with the large population of single people and leading to a large increase in demand for microwave dinners often found in store refrigerators with door handles that must be used by the customers.
Microwave dinners in store refrigerator with door handle that customers must use
Several other specific scenarios exist for rapid efficient spread of the virus through these giant retail stores.
Bus Service for “Essential” Workers and Others
Santa Clara County also has a bus service, the VTA or Valley Transportation Authority, in widespread use with patrons, often “essential workers,” sharing an enclosed space and seats.
VTA Bus in Operation on December 7, 2020, Santa Clara County, California
Giant Apartment Complexes are Common in Santa Clara County
The lockdown shelter in place and stay at home orders confine “non-essential workers” to numerous generally large apartment complexes, often with hundreds of tenants, possibly thousands in some cases. In Mountain View, California — site of Google’s headquarters — about fifty-eight percent of residents (Town Charts, see Figure 5) are renters, most in large complexes. These complexes feature shared trash chutes/rooms, laundry rooms, hallways and lobbies with exterior doors and fire doors that must be opened by hand in most cases, providing many shared surfaces and spaces for spread of the virus.
Typical Trash Chute Room with Fire Door in Santa Clara County — Note Door Handle (December 7, 2020)Typical Trash Room Interior with Trash Chute (Note Handle) in Santa Clara County (December 7, 2020)Typical Laundry Room Door with Handle in Santa Clara County (December 7, 2020)
Note that fire regulations require closely spaced closed fire doors in the interior hallways — with handles or knobs that all residents must use to open the fire doors.
The large apartment complexes common in Santa Clara County provide numerous shared spaces where aerosol virus particles can collect and linger in the air as well as shared surfaces such as door handles that all residents must touch.
Gloves are not required. Gloves would have to be handled carefully and sterilized before and after each or nearly each use to avoid spreading the virus, something probably impractical and certainly currently NOT done by most residents.
In general, the apartment complex support staff cannot clean each door handle after each use. The shared support staff themselves are a high risk of both becoming infected and spreading the infection to other residents. Almost none have training or experience in bio-safety measures.
Conclusion
Despite hyperbolic headlines and reasonable expectations, deaths attributed to COVID-19 have remained remarkably low in 2020, although that may — of course — change. We will see if the usual winter surge in cases and deaths from respiratory illnesses subsides for COVID-19 or not. Prediction is notoriously difficult — especially about the future. As demonstrated above, this appears to have been in spite of rather than because of the stay-at-home and lockdown measures.
The reasons for this remarkably low death rate in Santa Clara County in 2020 remain unknown. Possible explanations include the bright sunny climate — among the most pleasant in the world, close long term past contact with China contributing to a high pre-existing immunity or resistance to SARS type coronaviruses in general, some genetic or cultural difference in Santa Clara County’s heavily Asian population (death rates in Japan and other Asian nations have been quite low compared to the United States or Europe if official figures are to be believed), better treatment of patients such as avoiding intubation, higher consumption of vitamin D by the health conscious residents, or some other cause.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).