Short review of the Microclimate AIR anti-COVID “Space” Helmet
We do not receive any compensation for this review or use of the product reviewed. We recommend that you talk to your doctor or other health professional regarding use of this product, especially if you have any respiratory or other health problems.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Veteran science reporter Nicholas Wade has written a detailed accessible article on the origins of the COVID-19 pandemic and the evidence for and against a laboratory leak at the Wuhan Institute of Virology (WIV), arguing that the lab leak theory is more likely based on the available evidence.
Very little if any of this article is new but Wade presents the information in a clear way with a minimum of technical jargon. He properly acknowledges several prior detailed analyses and reports on the issues.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Veteran science reporter Nicholas Wade has written a detailed accessible article on the origins of the COVID-19 pandemic and the evidence for and against a laboratory leak at the Wuhan Institute of Virology (WIV), arguing that the lab leak theory is more likely based on the available evidence.
Very little if any of this is new but Wade presents the information in a clear way with a minimum of technical jargon. He properly acknowledges several prior detailed analyses and reports on the issues.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Antibody Dependent Enhancement (ADE) is a phenomenon that has been observed with a number of vaccines in which the vaccine initially produces no or negligible adverse effects but when the vaccinated person or animal actually encounters the virus or bacteria the vaccine is intended to stop, the immune system overreacts to the infection and harms or kills the vaccinated person. Prior to the COVID-19 pandemic, previous attempts to develop vaccines to prevent coronavirus infections such as SARS (2003, not SARS-COV-2) and MERS failed due to ADE.
How likely is potentially fatal antibody dependent enhancement (ADE) with the COVID-19 vaccines? Simple answer: we don’t know.We are conducting a gigantic uncontrolled experiment on a large fraction of the human race.
The Moderna clinical trials of their RNA COVID-19 vaccine, linked and discussed at the end of this article, suggest that ADE reactions in generally healthy persons similar to the test subjects in their trial are probably (95% confidence level) less than one in sixty-six (66) persons (1.5 percent) using the rule of three in statistics. This is based on a tiny sample of only 196 persons in the trial who actually developed COVID-19 — were actually exposed to the virus. ADE does not appear to have been reported in any of these 196 cases.
UPDATE (April 27, 2021): It is a bit unclear what number — 196, 11, or 185 — to use in the rule of three. The Moderna trial reported only eleven (11) vaccinated subjects with COVID-19 and 185 unvaccinated subjects with COVID-19. Thus, one could use the eleven in which case the rule of three would imply that the risk of ADE is probably less than one in 3.6. However, about 185 vaccinated subjects were exposed to COVID-19 in the vaccinated group as in the un-vaccinated control group. The vaccine worked for all but 11 of these. This would make the correct number 185 instead of 196 and give an estimate that the risk of ADE is probably (95% confidence level) less than one in sixty-one (1:61) or 1.6 percent. Most likely the correct number is about 185 (not the naive 196); the estimated bound on the risk is just about the same for 185 and 196.
References on Historical Failures of Coronavirus Vaccines due to ADE
VIII.For a vaccine to work, our immune system needs to be stimulated to produce a neutralizing antibody, as opposed to a non-neutralizing antibody. A neutralizing antibody is one that can recognize and bind to some region (‘epitope’) of the virus, and that subsequently results in the virus either not entering or replicating in your cells. A non-neutralizing antibody is one that can bind to the virus, but for some reason, the antibody fails to neutralize the infectivity of the virus. In some viruses, if a person harbors a non-neutralizing antibody to the virus, a subsequent infection by the virus can cause that person to elicit a more severe reaction to the virus due to the presence of the non-neutralizing antibody. This is not true for all viruses, only particular ones. This is called Antibody Dependent Enhancement (ADE), and is a common problem with Dengue Virus, Ebola Virus, HIV, RSV, and the family of coronaviruses. In fact, this problem of ADE is a major reason why many previous vaccine trials for other coronaviruses failed. Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place. This can cause a hyperinflammatory response, a cytokine storm, and a generally dysregulation of the immune system that allows the virus to cause more damage to our lungs and other organs of our body. In addition, new cell types throughout our body are now susceptible to viral infection due to the additional viral entry pathway. There are many studies that demonstrate that ADE is a persistent problem with coronaviruses in general, and in particular, with SARS-related viruses. ADE has proven to be a serious challenge with coronavirus vaccines, and this is the primary reason many of such vaccines have failed in early in-vitro or animal trials. For example, rhesus macaques who were vaccinated with the Spike protein of the SARS-CoV virus demonstrated severe acute lung injury when challenged with SARS-CoV, while monkeys who were not vaccinated did not. Similarly, mice who were immunized with one of four different SARS-CoV vaccines showed histopathological changes in the lungs with eosinophil infiltration after being challenged with… (EMPHASIS ADDED)
Specific references for failures of coronavirus vaccines for SARS (2003, not SARS-COV-2) and MERS are given after the following section on ADE and COVID-19/SARS-COV-2
This is a March 12, 2018 article from Children’s Health Defense (Robert F. Kennedy Jr’s group) with an overview of several cases of known or suspected antibody dependent enhancement in some vaccines with scientific references. Does not appear to discuss the coronavirus vaccine failures with ADE.
NOTE: many articles that turn up in searches now appear to omit or not clearly state that previous attempts to develop coronavirus vaccines failed due to ADE in early trials.
Abstract: Antibody-dependent enhancement (ADE) exists in several kinds of virus. It has a negative influence on antibody therapy for viral infection. This effect was first identified in dengue virus and has since also been described for coronavirus. To date, the rapid spread of the newly emerged coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causing coronavirus disease 2019 (COVID-19), has affected over 3.8 million people across the globe. The novel coronavirus poses a great challenge and has caused a wave of panic. In this review, antibody-dependent enhancements in dengue virus and two kinds of coronavirus are summarized. Possible solutions for the effects are reported. We also speculate that ADE may exist in SARS-CoV-2.
Keywords: Antibody-dependent enhancement (ADE); Coronavirus disease 2019 (COVID-19); Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); Severe acute respiratory syndrome coronavirus (SARS-CoV); Middle East respiratory syndrome coronavirus (MERS-CoV)
Highlights
Five mechanisms of antibody-dependent enhancement have been discussed to date, with the most frequent effect being related to FcγR.
Antibody-dependent enhancement has been discovered in both severe acute respiratory syndrome coronavirus and Middle East respiratory syndrome coronavirus, but the mechanism is not completely clear; different studies have led to different opinions.
Many scientist have mentioned the potential existence of antibody-dependent enhancement in the 2019 novel coronavirus – severe acute respiratory syndrome coronavirus.
The most recent studies on both convalescent plasma transmission and the application of inactivated vaccine did not report any case of antibody-dependent enhancement.
Yip MS, Leung NH, Cheung CY, et al. Antibody-dependent infection of human macrophages by severe acute respiratory syndrome coronavirus. Virol J. 2014;11:82. Published 2014 May 6. doi:10.1186/1743-422X-11-82 (PDF attached to this email)
Abstract
Background
Public health risks associated to infection by human coronaviruses remain considerable and vaccination is a key option for preventing the resurgence of severe acute respiratory syndrome coronavirus (SARS-CoV). We have previously reported that antibodies elicited by a SARS-CoV vaccine candidate based on recombinant, full-length SARS-CoV Spike-protein trimers, trigger infection of immune cell lines. These observations prompted us to investigate the molecular mechanisms and responses to antibody-mediated infection in human macrophages.
Methods
We have used primary human immune cells to evaluate their susceptibility to infection by SARS-CoV in the presence of anti-Spike antibodies. Fluorescence microscopy and real-time quantitative reverse transcriptase polymerase chain reaction (RT-PCR) were utilized to assess occurrence and consequences of infection. To gain insight into the underlying molecular mechanism, we performed mutational analysis with a series of truncated and chimeric constructs of fragment crystallizable γ receptors (FcγR), which bind antibody-coated pathogens.
Results
We show here that anti-Spike immune serum increased infection of human monocyte-derived macrophages by replication-competent SARS-CoV as well as Spike-pseudotyped lentiviral particles (SARS-CoVpp). Macrophages infected with SARS-CoV, however, did not support productive replication of the virus. Purified anti-viral IgGs, but not other soluble factor(s) from heat-inactivated mouse immune serum, were sufficient to enhance infection. Antibody-mediated infection was dependent on signaling-competent members of the human FcγRII family, which were shown to confer susceptibility to otherwise naïve ST486 cells, as binding of immune complexes to cell surface FcγRII was necessary but not sufficient to trigger antibody-dependent enhancement (ADE) of infection. Furthermore, only FcγRII with intact cytoplasmic signaling domains were competent to sustain ADE of SARS-CoVpp infection, thus providing additional information on the role of downstream signaling by FcγRII.
Conclusions
These results demonstrate that human macrophages can be infected by SARS-CoV as a result of IgG-mediated ADE and indicate that this infection route requires signaling pathways activated downstream of binding to FcγRII receptors.
Liu L, Wei Q, Lin Q, et al. Anti-spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection.JCI Insight. 2019;4(4):e123158. Published 2019 Feb 21. doi:10.1172/jci.insight.123158 (PDF too large to attach to email, available on web site linked above).
Abstract
Newly emerging viruses, such as severe acute respiratory syndrome coronavirus (SARS-CoV), Middle Eastern respiratory syndrome CoVs (MERS-CoV), and H7N9, cause fatal acute lung injury (ALI) by driving hypercytokinemia and aggressive inflammation through mechanisms that remain elusive. In SARS-CoV/macaque models, we determined that anti–spike IgG (S-IgG), in productively infected lungs, causes severe ALI by skewing inflammation-resolving response. Alveolar macrophages underwent functional polarization in acutely infected macaques, demonstrating simultaneously both proinflammatory and wound-healing characteristics. The presence of S-IgG prior to viral clearance, however, abrogated wound-healing responses and promoted MCP1 and IL-8 production and proinflammatory monocyte/macrophage recruitment and accumulation. Critically, patients who eventually died of SARS (hereafter referred to as deceased patients) displayed similarly accumulated pulmonary proinflammatory, absence of wound-healing macrophages, and faster neutralizing antibody responses. Their sera enhanced SARS-CoV–induced MCP1 and IL-8 production by human monocyte–derived wound-healing macrophages, whereas blockade of FcγR reduced such effects. Our findings reveal a mechanism responsible for virus-mediated ALI, define a pathological consequence of viral specific antibody response, and provide a potential target for treatment of SARS-CoV or other virus-mediated lung injury.
Keywords: Infectious disease, Pulmonology
Keywords: Cytokines, Immunoglobulins, Macrophages
ADE in Ferrets with SARS (2003, not SARS-COV-2)
NOTE: Ferrets have a similar respiratory system to humans and are often used for animal studies of vaccines for respiratory illnesses for this reason.
Weingartl H, Czub M, Czub S, et al. Immunization with modified vaccinia virus Ankara-based recombinant vaccine against severe acute respiratory syndrome is associated with enhanced hepatitis in ferrets. J Virol. 2004;78(22):12672-12676. doi:10.1128/JVI.78.22.12672-12676.2004
Abstract
Severe acute respiratory syndrome (SARS) caused by a newly identified coronavirus (SARS-CoV) is a serious emerging human infectious disease. In this report, we immunized ferrets (Mustela putorius furo) with recombinant modified vaccinia virus Ankara (rMVA) expressing the SARS-CoV spike (S) protein. Immunized ferrets developed a more rapid and vigorous neutralizing antibody response than control animals after challenge with SARS-CoV; however, they also exhibited strong inflammatory responses in liver tissue. Inflammation in control animals exposed to SARS-CoV was relatively mild. Thus, our data suggest that vaccination with rMVA expressing SARS-CoV S protein is associated with enhanced hepatitis.
Deming D, Sheahan T, Heise M, Yount B, Davis N, et al. (2006) Vaccine Efficacy in Senescent Mice Challenged with Recombinant SARS-CoV Bearing Epidemic and Zoonotic Spike Variants . PLOS Medicine 3(12): e525. https://doi.org/10.1371/journal.pmed.0030525
In 2003, severe acute respiratory syndrome coronavirus (SARS-CoV) was identified as the etiological agent of severe acute respiratory syndrome, a disease characterized by severe pneumonia that sometimes results in death. SARS-CoV is a zoonotic virus that crossed the species barrier, most likely originating from bats or from other species including civets, raccoon dogs, domestic cats, swine, and rodents. A SARS-CoV vaccine should confer long-term protection, especially in vulnerable senescent populations, against both the 2003 epidemic strains and zoonotic strains that may yet emerge from animal reservoirs. We report the comprehensive investigation of SARS vaccine efficacy in young and senescent mice following homologous and heterologous challenge.
Methods and Findings
Using Venezuelan equine encephalitis virus replicon particles (VRP) expressing the 2003 epidemic Urbani SARS-CoV strain spike (S) glycoprotein (VRP-S) or the nucleocapsid (N) protein from the same strain (VRP-N), we demonstrate that VRP-S, but not VRP-N vaccines provide complete short- and long-term protection against homologous strain challenge in young and senescent mice. To test VRP vaccine efficacy against a heterologous SARS-CoV, we used phylogenetic analyses, synthetic biology, and reverse genetics to construct a chimeric virus (icGDO3-S) encoding a synthetic S glycoprotein gene of the most genetically divergent human strain, GDO3, which clusters among the zoonotic SARS-CoV. icGD03-S replicated efficiently in human airway epithelial cells and in the lungs of young and senescent mice, and was highly resistant to neutralization with antisera directed against the Urbani strain. Although VRP-S vaccines provided complete short-term protection against heterologous icGD03-S challenge in young mice, only limited protection was seen in vaccinated senescent animals. VRP-N vaccines not only failed to protect from homologous or heterologous challenge, but resulted in enhanced immunopathology with eosinophilic infiltrates within the lungs of SARS-CoV–challenged mice. VRP-N–induced pathology presented at day 4, peaked around day 7, and persisted through day 14, and was likely mediated by cellular immune responses.
Conclusions
This study identifies gaps and challenges in vaccine design for controlling future SARS-CoV zoonosis, especially in vulnerable elderly populations. The availability of a SARS-CoV virus bearing heterologous S glycoproteins provides a robust challenge inoculum for evaluating vaccine efficacy against zoonotic strains, the most likely source of future outbreaks.
FINAL COMMENT
How likely is potentially fatal antibody dependent enhancement (ADE) with the COVID-19 vaccines? Simple answer: we don’t know. We are conducting a gigantic uncontrolled experiment on a large fraction of the human race.
These are the trial results reported by Moderna for their now widely used RNA vaccine.
The emergency use authorization for the Moderna vaccine was based on a study of 14,134 test subjects who actually received the vaccine and not the placebo. ADE requires both being vaccinated and exposure to the virus. The Moderna study did not involve deliberately exposing the roughly 28,000 test subjects (both placebo and actually vaccinated) to SARS-COV-2. Rather the study waited for natural infection of the test subjects — a tiny number:
The median length of follow up for efficacy for participants in the study was 9 weeks post Dose 2. There were 11 COVID‑19 cases in the Moderna COVID‑19 Vaccine group and 185 cases in the placebo group, with a vaccine efficacy of 94.1% (95% confidence interval of 89.3% to 96.8%).
(from Moderna web site on April 21, 2021)
The Emergency Use Authorization (not standard FDA approval which takes years) was based on a total of 196 COVID-19 cases. Presumably these 196 patients did not exhibit ADE. Test subjects in these clinical trials for vaccine approvals — or emergency use authorization in this case — are generally quite healthy and are not a representative sample of the frail elderly at most risk from COVID-19. Thus the risk of ADE in generally healthy vaccinated persons similar to the test subjects used in the Moderna clinical trial is probably (95% confidence level) less than one in sixty-six (66) persons (1.5 percent) using the rule of three in statistics.
UPDATE (April 27, 2021): It is a bit unclear what number — 196, 11, or 185 — to use in the rule of three. The Moderna trial reported only eleven (11) vaccinated subjects with COVID-19 and 185 unvaccinated subjects with COVID-19. Thus, one could use the eleven in which case the rule of three would imply that the risk of ADE is probably less than one in 3.6. However, about 185 vaccinated subjects were exposed to COVID-19 in the vaccinated group as in the un-vaccinated control group. The vaccine worked for all but 11 of these. This would make the correct number 185 instead of 196 and give an estimate that the risk of ADE is probably (95% confidence level) less than one in sixty-one (1:61) or 1.6 percent. Most likely the correct number is about 185 (not the naive 196); the estimated bound on the risk is just about the same for 185 and 196.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
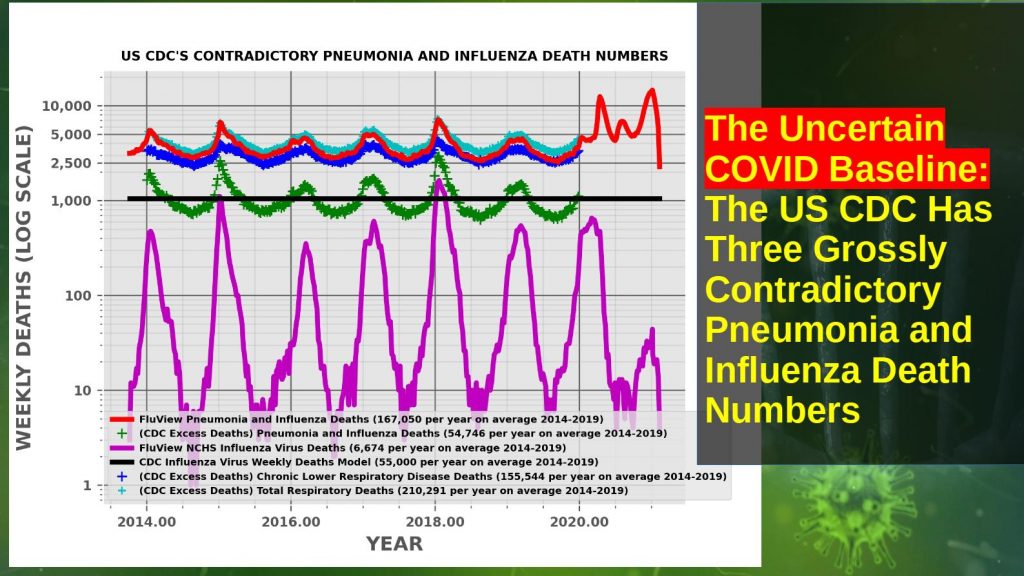
US CDC’s Contradictory Pneumonia and Influenza Weekly Death Numbers 2014-2019
The United States Centers for Disease Control (CDC) has at least three different, grossly contradictory historical pneumonia and influenza death numbers. The CDC FluView pneumonia and influenza pre-COVID death number is OVER THREE TIMES the leading causes of death number. Pneumonia and influenza are often conflated in the CDC’s documentation and in the CDC’s influenza death model.
These death numbers are frequently used as the baseline for comparison of the COVID-19 death numbers and assessing the severity of the pandemic relative to previous years and pandemics such as the 1957, 1968, and 2009 influenza pandemics.
The Three Different Sets of Pneumonia and Influenza Death Numbers
Leading Causes of Death Pneumonia and Influenza (P&I) Deaths (About 55,000 per year)
FluView Pneumonia and Influenza (P&I) Deaths (About 167,000 pre-COVID, Over THREE TIMES Leading Causes of Death, About 7,000 Influenza Virus Deaths Per Year)
CDC Model Influenza Virus Deaths (About 55,000 per year, at least THREE TIMES FluView Influenza Deaths)
This is the program and data files used to generate the plot above comparing the CDC’s pneumonia and influenza death numbers from 2014 through 2019. Download and use the 7-Zip or other file archiver for MS Windows or the Unix command tar -xvf cdc_numbers.tar to unpack the program and data files.
This Python 3 program generates a plot comparing the different numbers on a log scale for easy comparison.
The program also plots the weekly deaths for “chronic lower respiratory disease,” mostly chronic bronchitis and emphysema — also referred to as “chronic obstructive pulmonary disease” in the medical literature. It is likely that the THREE TIMES LARGER FluView pneumonia and influenza death numbers are produced by borrowing deaths from chronic lower respiratory disease (mostly chronic bronchitis and emphysema) and adding them to the “pneumonia and influenza” deaths reported in the leading causes of death report.
discusses these issues in much more detail and provides references and links.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The United States Centers for Disease Control (CDC) has at least three different, grossly contradictory historical pneumonia and influenza death numbers. Pneumonia and influenza are often conflated in the CDC’s documentation and influenza death model. These death numbers are frequently used as the baseline for comparison of COVID-19 death numbers and assessing the severity of the pandemic relative to previous years and influenza pandemics.
Leading Causes of Death Pneumonia and Influenza (P&I) Deaths (About 55,000 per year)
FluView Pneumonia and Influenza (P&I) Deaths (About 188,000 pre-COVID, Over THREE TIMES Leading Causes of Death, About 5-15,000 Influenza Deaths Per Year)
CDC Model Influenza Only Deaths (About 55,000 per year, at least THREE TIMES FluView Influenza Deaths)
This video discusses these different contradictory numbers and their implications for the COVID-19 pandemic.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This article argues that the US Centers for Disease Control (CDC)’s April 2020 guidance for filling out death certificates for possible COVID-19 related deaths strongly encourages, if not requires, assigning COVID-19 as the underlying cause of death (UCOD) in any death where COVID-19 or the SARS-COV-2 virus may be present, which appears to differ from common historical practice for pneumonia and influenza deaths where pneumonia was frequently treated as a “complication,” a cause of death but not the underlying cause of death.
This means the number of COVID deaths should be compared to a count of death certificates where pneumonia and influenza were listed as a cause of death or even a lesser contributing factor, a historical number which appears to have been at least 188,000 per year based on the CDC FluView web site. The proper comparison number may be even larger if deaths that historically were listed as heart attacks, cancer or other causes than pneumonia or influenza are also being reassigned due to the April 2020 guidance.
The CDC has at least three different historical pneumonia and influenza death numbers. These are the leading causes of death report numbers of about 55,000 deaths per year which appears based on death certificates, a poorly documented mathematical/computer model which attributes about 55,000 deaths per year with a large error to the influenza virus, and the FluView web site which attributed about 188,000 deaths per year to pneumonia and influenza.
The leading causes of death historical numbers appear based on the underlying cause of death listed on the death certificate whereas the FluView historical numbers appear based on death certificates that list pneumonia or influenza as a cause of death, in most cases not the underlying cause of death. The historical FluView death numbers appear to be the proper baseline for comparison to COVID-19, although an even larger number is possible if there has been practically significant reassignment of heart attacks and other deaths as well.
This would mean that COVID-19 is less deadly than popular perceptions based frequently on comparisons to “flu death numbers” of about 55,000 per year apparently derived either from the CDC’s leading causes of death report or the influenza virus model.
Note that this is not a claim that COVID-19 or SARS-COV-2 plays no causal role in the deaths: a death “with” COVID rather than a death “due to” COVID in popular debates. Rather, the proper interpretation is probably that COVID-19 acts predominantly as an opportunistic infection instead of an inherently deadly infection able to easily kill healthy young people with a strong immune system. Vaccines are likely to have small or no ability to prevent death from an opportunistic infection since the infected vaccinated person will have a weak or failed immune system with little or no ability to produce the immune response learned from the vaccination.
The language and numbers on the CDC web sites and official reports and documents are remarkably confusing and grossly contradictory in some cases — such as the historical number of deaths attributed to pneumonia and influenza which differs by over a factor of THREE. Error bars or confidence levels on most numbers such as the death numbers are not reported as required by common scientific and engineering practice. These practices have been harshly criticized for years by scientists and medical experts such as Peter Doshi. Consequently it is impossible to make definite statements about the meaning of the numbers and the definitions of measured quantities discussed below.
This is a complex life-and-death subject with many nuances. Each section below expands each key point in detail, discussing the nuances and unknowns. Some facts and arguments are repeated in different sections for clarity.
Three Different Historical Pneumonia and Influenza Death Numbers
The United States Centers for Disease Control (CDC) documents and web site present at least THREE different historical (pre-2020) estimates of deaths from “influenza and pneumonia,” “pneumonia and influenza,” and/or “influenza” or the “flu” presumably meaning the influenza category of viruses. Which of these three death numbers, one of which differs by a factor of OVER THREE from the other two, should be compared to COVID-19 deaths? Indeed, it could well be incorrect to compare any of them to the COVID-19 deaths.
These three pneumonia and influenza death numbers are the value in the annual leading causes of death report — about 55,000 deaths each year, the tables of “pneumonia and influenza” (abbreviated as P&I) from the National Center for Health Statistics (NCSH) used on the FluView web site — about 188,000 deaths per year, OVER THREE TIMES the leading causes of death number, and the output of a poorly documented model of deaths attributed to the influenza category of viruses, a broad range centered at about 55,000 deaths per year.
Deaths attributed to COVID-19 in 2020 have frequently been compared to an estimate of about 55,000, either to the date of the report or for the entire year. The language used is often unclear but appears to refer to either the CDC’s influenza mathematical model or the leading causes of death number, which are similar numbers but technically not the same.
This article argues that the current COVID-19 death numbers are best compared to the larger FluView numbers, although an even larger different number may be appropriate if deaths that would have been attributed to heart attacks, strokes, or other blood coagulation related disorders in the absence of a positive SARS-COV-2 test or diagnosis are included in the current COVID-19 death counts.
The CDC FluView Web Site
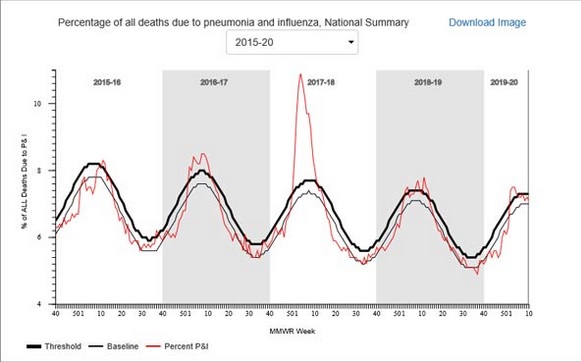
The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluViewPneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list about 188,000 deaths per year attributed to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
Note also that deaths attributed to “pneumonia and influenza” on the FluView web site are highly seasonal. A substantial increase over the summer is expected during the winter (or rainy season in Northern California and similar regions), peaking in December and January each year.
Also note that the seasonal variation is sinusoidal — like the oscillation of a pendulum or a mechanical spring. Contrary to popular culture, there is no clear step up when schools open in the fall or step down when schools close for the summer. It looks very much like something driven by the Sun, directly or indirectly by some mechanism or mechanisms. Possible mechanisms include Vitamin D production from sunlight, destruction of viruses and bacteria in the air or on surfaces by ultraviolet light in sunlight, general health benefits of a warm environment, or some other Sun-driven phenomenon.
The Leading Causes of Death Report
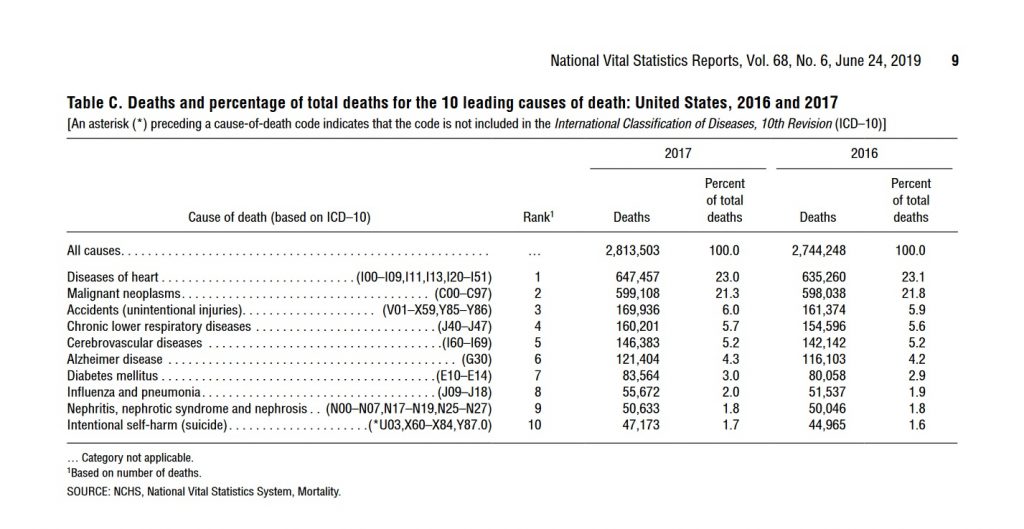
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
A longer, more detailed discussion of the FluView, leading causes of death, and the CDC’s influenza virus death model death numbers (yet another number) may be found below. It appears likely the FluView death numbers are defined similarly to current COVID-19 death counts; the reasons for this are explained in some detail.
Which Pneumonia and Influenza Death Numbers Should Be Compared to the COVID-19 Death Numbers?
The FluView and Leading Causes of Death numbers for “pneumonia and influenza” differ by a factor of OVER THREE. Note that both the FluView and Leading Causes of Death numbers have no error bars or error estimates given, implying exact numbers in common scientific and engineering practice. Should the number of COVID-19 deaths be compared to the FluView number or the leading causes of death number or some other number?
The CDC also uses a poorly documented mathematical model that attributes roughly 55,000 deaths from pneumonia and influenza to the influenza virus as the underlying cause, a number roughly comparable to the total pneumonia and influenza deaths in the leading causes of death. The influenza virus is confirmed by laboratory tests in only a small fraction of pneumonia and influenza deaths, about 6,000 per year.
Although the language is often unclear in the CDC documents and web site, the CDC appears to claim that an initial influenza infection which disappears or becomes undetectable in laboratory tests leads to the subsequent pneumonia, presumably a bacterial pneumonia although other viruses would be consistent with some lab tests. Based on this argument, the CDC appears to attribute most pneumonia deaths where historically pneumonia was listed as the “underlying cause of death” to the influenza virus for which there is a flu vaccine that the CDC promotes heavily — even though laboratory tests frequently fail to confirm influenza or even detect other viruses or bacteria instead. The “underlying cause of death” is discussed in more detail below.
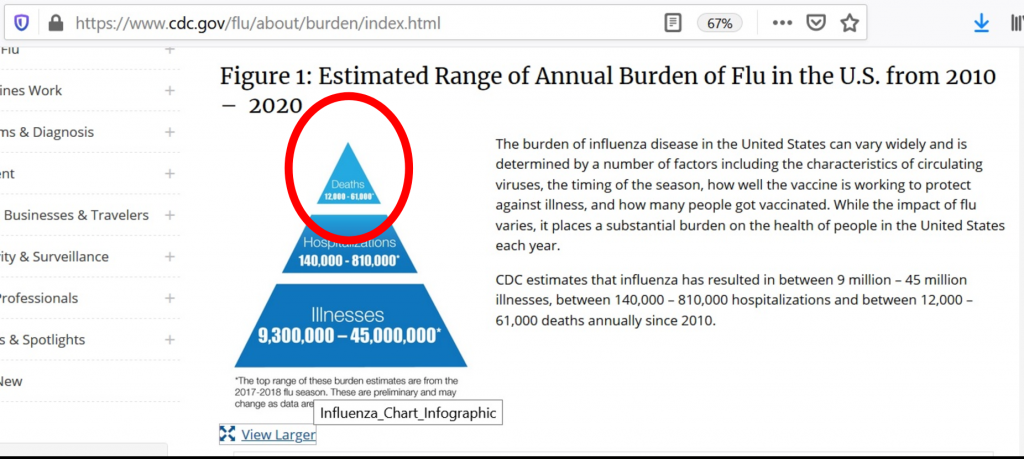
As shown in the graphic above, the CDC web site Disease Burden of Influenza (Figure 1) appears to give a range from 12,000 to 61,000 influenza deaths from this model. The graphic does not indicate if this range is a 95 percent confidence interval — a common scientific and engineering practice — or some other error estimate. The range in the graphic does not appear to match any of the 95 percent confidence levels for estimated deaths attributed to influenza in Table 1.
The History of Serious Criticism of the CDC’s “Flu” Death Numbers
There is a long history of serious criticism of the CDC’s “flu” death numbers by medical scientists and others. The most prominent critic is Peter Doshi, currently a professor at the University of Maryland and an associate editor at the British Medical Journal.
Citing the results of actual laboratory tests of deceased patients, critics of the CDC’s flu death numbers such as University of Maryland Professor Peter Doshi have argued that pneumonia deaths are due to a range of different viruses, bacteria, other pathogens, and even toxins, rather than predominantly influenza as implied by the CDC’s influenza deaths model. The output of this model appears to be the basis of the baseline “flu” deaths numbers used in most popular and public policy discussions of COVID-19 deaths — although the leading causes of death report number may also be used.
The Reason for the Large Difference Between the FluView and Leading Causes of Death Numbers
The US CDC documents and web site are frequently unclear and even contradictory as in the case of these grossly contradictory totals of deaths from pneumonia and influenza. This makes it difficult to be certain of the cause for the difference. Nonetheless, the technical notes for each document — FluView and the leading causes of death — give a highly probable reason.
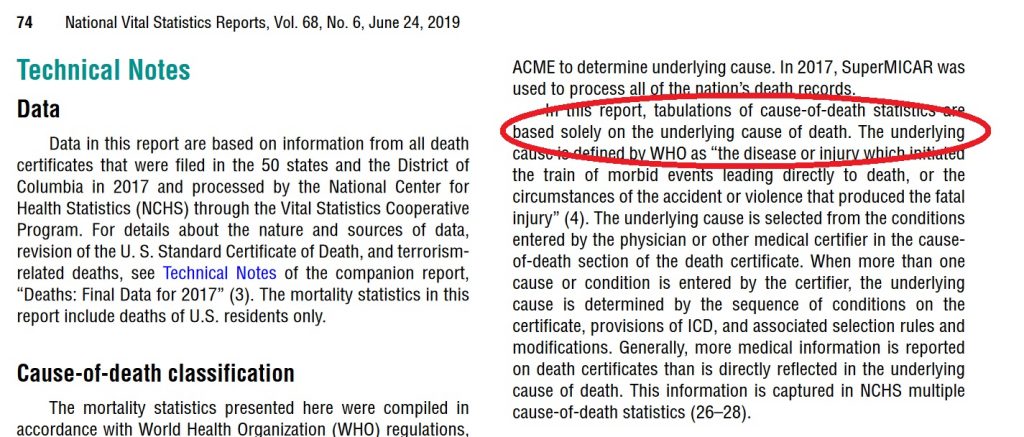
Leading Causes of Death Report for 2017 with “the underlying cause of death” language circled in red. (Dec. 18, 2020)
Death certificates frequently have multiple causes of death. One of these is assigned as the underlying cause of death. This may be quite arbitrary in some cases. Indeed the concept of “underlying cause of death” may not be well defined for some deaths because the aged may develop multiple health problems in parallel that are fatal in combination.
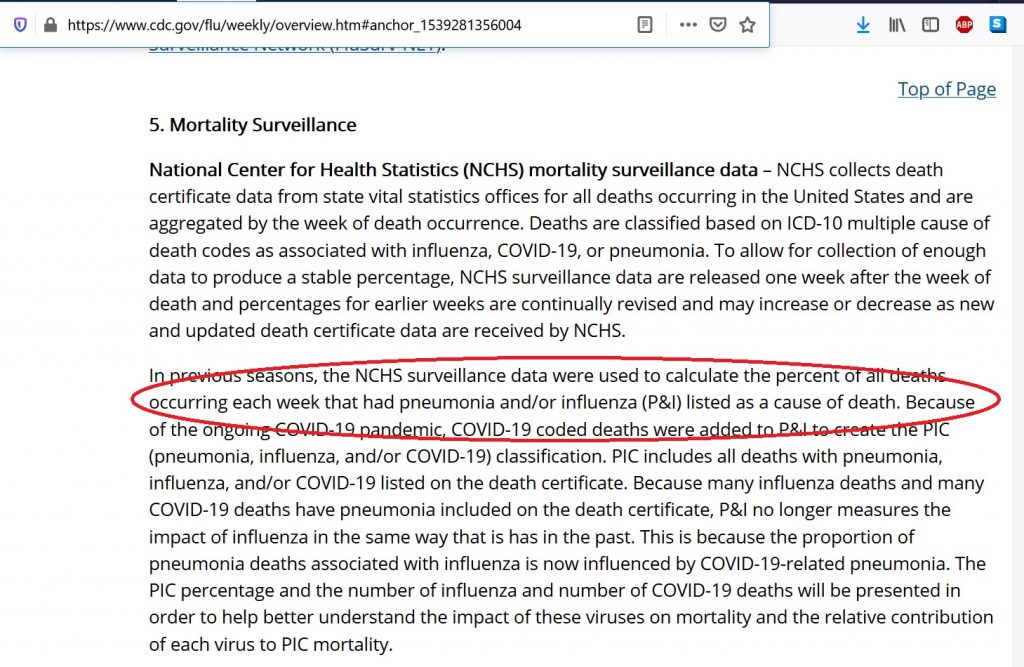
FluView Mortality Surveillance notes with “A Cause of Death” Language Circled in Red (Dec. 18, 2020)
The Rules for Assigning the Underlying Cause of Death Before COVID-19
Prior to 2020 and COVID-19, most pneumonia deaths did not list pneumonia or the pneumonia-causing pathogen if known as the underlying cause of death. This will be discussed in detail below. The only common partial exception was HIV/AIDS where pneumocystis carinii pneumonia (a common fungus) was often the immediate cause of death and the Human Immunodeficiency Virus (HIV) is almost always listed as the underlying cause of death. However, HIV is not the pneumonia-causing pathogen which is the pneumocystis fungus. Instead, most pneumonia deaths, those included in the FluView numbers but not included in the leading causes of death numbers, were attributed to a cause such as a chronic lower respiratory disease, heart disease, cancer, even accidents, and other usually pre-existing conditions as the underlying cause of death.
The CDC follows the World Health Organization (WHO)’s definition of the underlying cause of death. WHO defines the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury” in accordance with the rules of the International Classification of Diseases (ICD).
In the United States, the underlying cause of death is listed last in the list of causes of death in part I of the death certificate. The immediate cause of death is listed first. Part 2 lists other conditions that are considered contributing factors but somehow not causes. Pneumonia is often the immediate cause of death in part 1 of the death certificate.
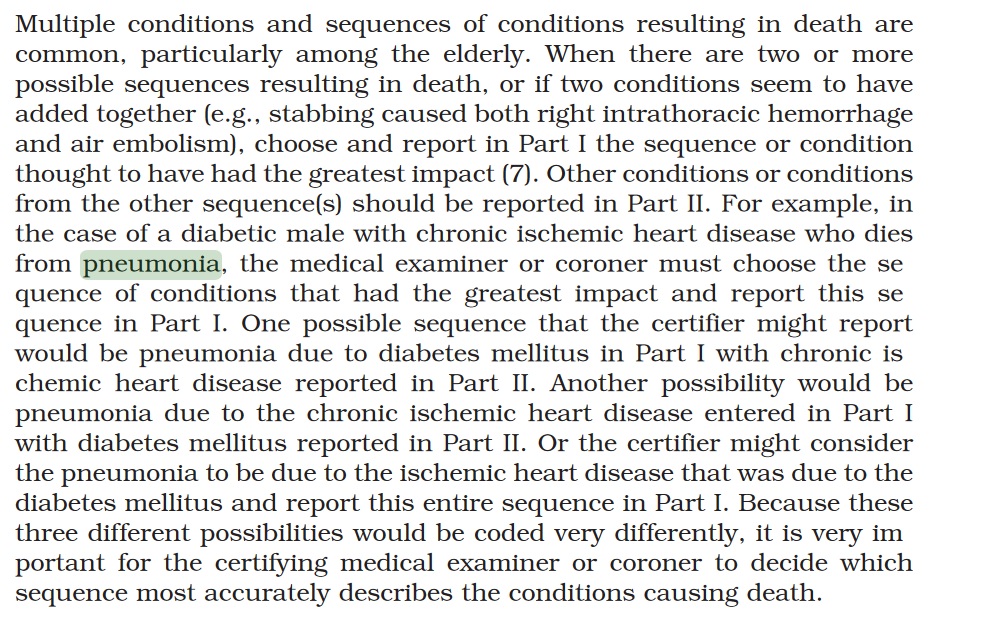
In principle, death certificates and the assignment of causes of death including the underlying cause of death is governed or at least guided by the CDC’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (2003 Revision). This one-hundred and thirty-eight (138) page manual actually provides very limited guidance on how to assign the underlying cause of death in cases where pneumonia is present. Page twenty-five (25) has the only detailed discussion of deaths involving pneumonia:
US CDC Medical Examiners’ Handbook 2003 suggests attributing a pneumonia death to either chronic ischemic heart disease or diabetes mellitus as the underlying cause but not the pneumonia or pneumonia-causingpathogen. No clear direction to the physician.
Pneumonia is often a nonspecific process that occurs as the terminal event in someone who dies of a more specific underlying cause of death, such as congestive heart failure resulting from ischemic heart disease. In such cases, the specific underlying cause of death should be included in the cause-of-death statement.
Pneumonia is often designated as either community acquired or hospital or institution acquired (nosocomial). If the community- or institution-acquired nature of the pneumonia is known, the cause-of-death statement should include an indication of which one applies.
The specific bacterial, viral, or other infectious agent, if known, should be cited in the cause-of-death statement.
Relevant risk factors should also be cited in the cause-of-death statement, as might occur in an alcoholic who develops tuberculous pneumonia. Only in those instances where pneumonia has caused death and there is no known underlying cause or risk factor should the underlying cause of death be stated as “Pneumonia,” being sure to specify the infectious agent, if known, or specifying that a specific etiology is unknown, if such is the case.
Emphasis Added
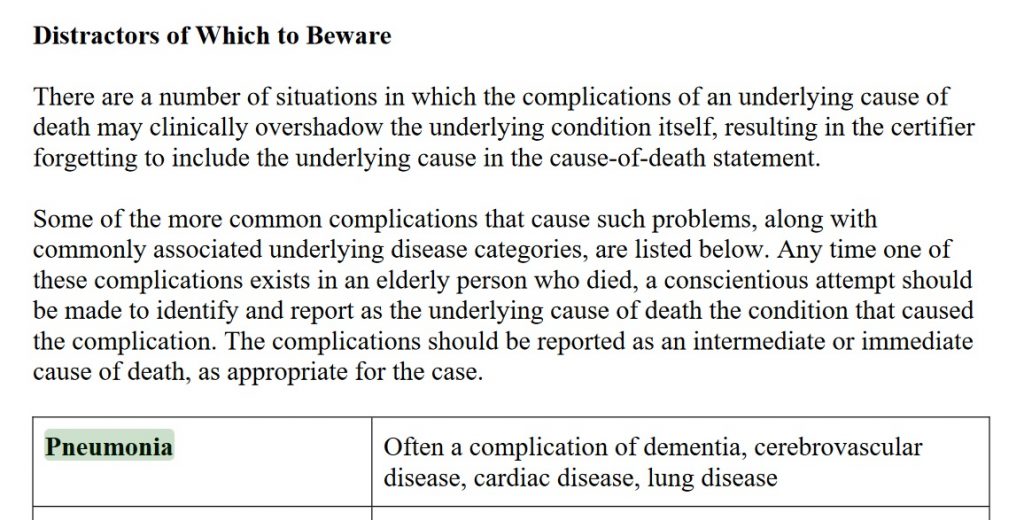
And on page 113 of Cause of Death and the Death Certificate by Randy Hanzlick, dementia, cerebrovascular disease, cardiac disease, and lung disease are all listed as common underlying causes of death in cases of deaths due to pneumonia:
Thus, traditionally, pre-2020 and COVID-19, pneumonia deaths were frequently assigned a non-pneumonia underlying cause of death, usually a pre-existing condition and not the pneumonia-causing pathogen such as the influenza virus or SARS-COV-2, in common medical practice. Based on the technical notes these pneumonia and influenza deaths would be included in the FluView death numbers but not in the leading causes of death report.
Comparing COVID-19 Death Numbers to the Pneumonia and Influenza Death Numbers and Estimates from Previous Years
As shown above, the CDC has at least three (3) different pneumonia and influenza death numbers and estimates: the Leading Causes of Death Report (about 55,000 deaths per year, about two percent of annual deaths from all causes), the FluView graph and underlying data from the NCHS (about 188,000 deaths per year, six to ten percent of annual deaths from all causes, before 2020), and the influenza death model estimates that range from 12,000 to 61,000 deaths per year with the best estimate close to the number of pneumonia and influenza deaths in the leading causes of death report. Are any of these the proper baseline for comparing COVID-19 deaths to prior years or should some other number or estimate be used?
In the absence of the RT-PCR and antibody tests for the SARS-COV-2 virus, most COVID-19 deaths would have been unexplained pneumonia deaths lacking a laboratory test confirming influenza or other known pathogen. Possibly, some COVID-19 deaths would have been listed as heart attacks or strokes, those COVID-19 deaths attributed to the blood clots and other blood-related anomalies currently blamed on COVID-19, or even some other causes. The rest of this article will focus on the pneumonia deaths which would probably comprise most of the COVID-19 deaths in the absence of laboratory tests.
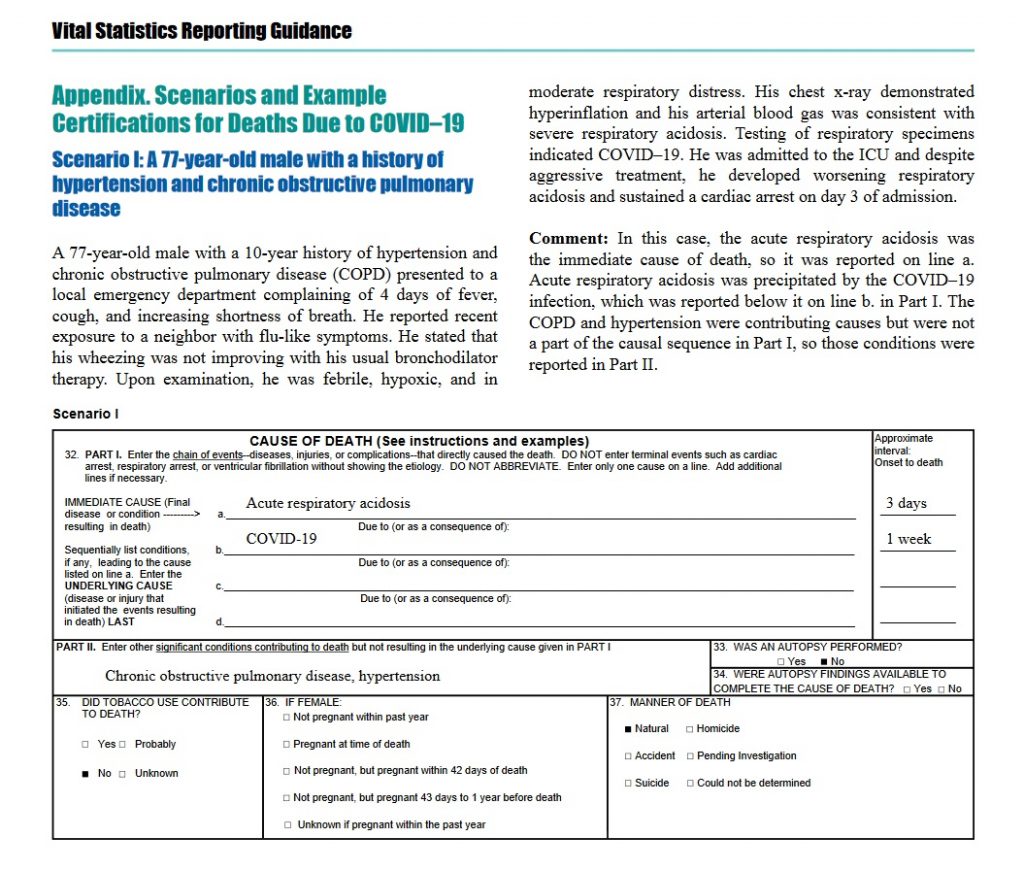
The US CDC’s April 2020 guidelines for reporting COVID-19 deaths clearly direct physicians and others not to list chronic obstructive pulmonary disease (COPD) as the underlying cause of death in COVID-19 cases, moving it to Part 2 of the death certificate reserved for “non-cause” contributing factors, which differs dramatically from medical practice prior to 2020 as described in Randy Hanzlick’s book and implicit in the FluView pneumonia and influenza deaths data.
In some cases, survival from COVID–19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID–19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II and not in Part I.
This guidance also gives a specific example of a COVID-19 death with COPD relegated to Part 2:
COVID-19 Death Guidance Example with COPD as Contributing Factor Only
Although other causes of death that are often given as the underlying cause of death in pneumonia cases on pre-2020 death certificates are not explicitly identified in the April 2020 guidance document, it seems probable most physicians would move these pre-existing conditions to Part 2 and not list them as the underlying cause of death for COVID-19 based on the April 2020 CDC guidance document. Note that COPD would fall under the category “lung disease” in the list below from Randy Hanzlick’s Causes of Death and the Death Certificate:
Thus, COVID-19 deaths since the April 2020 guidance are probably roughly comparable to the FluView deaths, the larger number, the 188,000 pneumonia and influenza deaths per year. The language “roughly” is used because the April 2020 guidance appears to strongly encourage physicians and others to assign COVID-19 as the underlying cause of death in any death where COVID-19 is detected by tests or perhaps even just suspected, raising the possibility that heart attack and stroke deaths might be wrongly classified as COVID-19 deaths as well as the traditional pneumonia and influenza deaths that would be listed in the FluView data. These would presumably be misclassified as the COVID-19 deaths exhibiting the mysterious blood clots and other blood-related problems reported in some COVID-19 cases and deaths. Thus, the FluView death numbers may represent a lower bound on COVID-19 deaths rather than an exact baseline — unfortunately.
Ealy et al have raised the question whether the CDC complied with the Paperwork Reduction Act (PRA) and Information Quality Act (IQA) requirements in issuing the April and earlier March COVID-19 death certification guidelines, apparently without submitting these for public comment through the Federal Register as Ealy and co-authors claim is required by these federal laws.
Conclusion
Thus, due to the guidance on the death certificates from the CDC in April 2020, COVID-19 deaths on death certificates appear comparable to the larger FluView death numbers — or even larger numbers if heart attacks, strokes or other blood coagulation related deaths with a positive test or clinical diagnosis are being classified as COVID-19 deaths.
The CDC’s documents and web site are remarkably unclear, contradictory, and confusing for public health and scientific information presented to the general public, busy doctors and other medical professionals, or even research scientists — as previously noted by Peter Doshi and others.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Many Seeming Routes for Efficient Spread of COVID-19 in Santa Clara County, California (USA)
Twenty minute video on many seeming routes for efficient spread of COVID-19 in Santa Clara County, California, USA (Silicon Valley). Discusses herding of residents into Big Box retail stores such as Safeway, Target, and Walmart, large apartment complexes, the VTA bus system, and construction projects with many shared spaces and surfaces.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The United States Centers for Disease Control (CDC) documents and web site present at least THREE different historical (pre-2020) estimates of deaths from “influenza and pneumonia,” “pneumonia and influenza,” and/or “influenza” or the “flu” presumably meaning the influenza category of viruses. Which of these three death numbers, one of which differs by a factor of OVER THREE from the other two, should be compared to COVID-19 deaths? Indeed, it could well be incorrect to compare any of them to the COVID-19 deaths.
These three pneumonia and influenza death numbers are the value in the annual leading causes of death report — about 55,000 deaths each year, the tables of “pneumonia and influenza” (abbreviated as P&I) from the National Center for Health Statistics (NCSH) used on the FluView web site — about 188,000 deaths per year, OVER THREE TIMES the leading causes of death number, and the output of a mysterious model of deaths attributed to the influenza category of viruses, a broad range centered at about 55,000 deaths per year.
Deaths attributed to COVID-19 in 2020 have frequently been compared to an estimate of about 55,000, either to the date of the report or for the entire year. The language used is often unclear but appears to refer to either the CDC’s influenza mathematical model or the leading causes of death number, which are similar numbers but technically not the same.
This article argues that the current COVID-19 death numbers are best compared to the larger FluView numbers, although an even larger different number may be appropriate if deaths that would have been attributed to heart attacks, strokes, or other blood coagulation related disorders in the absence of a positive SARS-COV-2 test or diagnosis are included in the current COVID-19 death counts.
The CDC FluView Web Site
The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluView Pneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list about 188,000 deaths per year attributed to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
Note also that deaths attributed to “pneumonia and influenza” on the FluView web site are highly seasonal. A substantial increase over the summer is expected during the winter (or rainy season in Northern California and similar regions), peaking in December and January each year.
Also note that the seasonal variation is sinusoidal — like the oscillation of a pendulum or a mechanical spring. Contrary to popular culture, there is no clear step up when schools open in the fall or step down when schools close for the summer. It looks very much like something driven by the Sun, directly or indirectly by some mechanism or mechanisms. Possible mechanisms include Vitamin D production from sunlight, destruction of viruses and bacteria in the air or on surfaces by ultraviolet light in sunlight, general health benefits of a warm environment, or some other Sun-driven phenomenon.
The Leading Causes of Death Report
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
A longer, more detailed discussion of the FluView, leading causes of death, and the CDC’s influenza virus death model death numbers (yet another number) may be found below. It appears likely the FluView death numbers are defined similarly to current COVID-19 death counts; the reasons for this are explained in some detail.
US CDC Leading Causes of Death Report Attributes Only About Two Percent of All Deaths to Pneumonia and Influenza (Line Item 8: Influenza and Pneumonia) — not the Six to Ten Percent in the FluView Graphs
Which Pneumonia and Influenza Death Numbers Should Be Compared to the COVID-19 Death Numbers?
The FluView and Leading Causes of Death numbers for “pneumonia and influenza” differ by a factor of OVER THREE. Note that both the FluView and Leading Causes of Death numbers have no error bars or error estimates given, implying exact numbers in common scientific and engineering practice. Should the number of COVID-19 deaths be compared to the FluView number or the leading causes of death number or some other number?
The CDC also uses a mysterious mathematical model that attributes roughly 55,000 deaths from pneumonia and influenza to the influenza virus as the underlying cause, a number roughly comparable to the total pneumonia and influenza deaths in the leading causes of death. The influenza virus is confirmed by laboratory tests in only a small fraction of pneumonia and influenza deaths, about 6,000 per year.
Although the language is often unclear in the CDC documents and web site, the CDC appears to claim that an initial influenza infection which disappears or becomes undetectable in laboratory tests leads to the subsequent pneumonia, presumably a bacterial pneumonia although other viruses would be consistent with some lab tests. Based on this argument, the CDC appears to attribute most pneumonia deaths where historically pneumonia was listed as the “underlying cause of death” to the influenza virus for which there is a flu vaccine that the CDC promotes heavily — even though laboratory tests frequently fail to confirm influenza or even detect other viruses or bacteria instead. The “underlying cause of death” is discussed in more detail below.
As shown in the graphic above, the CDC web site Disease Burden of Influenza (Figure 1) appears to give a range from 12,000 to 61,000 influenza deaths from this model. The graphic does not indicate if this range is a 95 percent confidence interval — a common scientific and engineering practice — or some other error estimate. The range in the graphic does not appear to match any of the 95 percent confidence levels for estimated deaths attributed to influenza in Table 1.
The History of Serious Criticism of the CDC’s “Flu” Death Numbers
There is a long history of serious criticism of the CDC’s “flu” death numbers by medical scientists and others. The most prominent critic is Peter Doshi, currently a professor at the University of Maryland and an associate editor at the British Medical Journal.
Citing the results of actual laboratory tests of deceased patients, critics of the CDC’s flu death numbers such as University of Maryland Professor Peter Doshi have argued that pneumonia deaths are due to a range of different viruses, bacteria, other pathogens, and even toxins, rather than predominantly influenza as implied by the CDC’s influenza deaths model. The output of this model appears to be the basis of the baseline “flu” deaths numbers used in most popular and public policy discussions of COVID-19 deaths — although the leading causes of death report number may also be used.
Why the Large Difference Between the FluView and Leading Causes of Death Numbers
The US CDC documents and web site are frequently unclear and even contradictory as in the case of these grossly contradictory totals of deaths from pneumonia and influenza. This makes it difficult to be certain of the cause for the difference. Nonetheless, the technical notes for each document — FluView and the leading causes of death — give a highly probable reason.
Leading Causes of Death Report for 2017 with “the underlying cause of death” language circled in red. (Dec. 18, 2020)
Death certificates frequently have multiple causes of death. One of these is assigned as the underlying cause of death. This may be quite arbitrary in some cases. Indeed the concept of “underlying cause of death” may not be well defined for some deaths because the aged may develop multiple health problems in parallel that are fatal in combination.
In contrast, the FluView site, the much larger number of deaths, appears to count deaths where pneumonia or influenza is listed as “a cause of death,” even if it is not the “underlying cause of death.”
FluView Mortality Surveillance notes with “A Cause of Death” Language Circled in Red (Dec. 18, 2020)
The Rules for Assigning the Underlying Cause of Death Before COVID-19
Prior to 2020 and COVID-19, most pneumonia deaths did not list pneumonia or the pneumonia-causing pathogen if known as the underlying cause of death. This will be discussed in detail below. The only common partial exception was HIV/AIDS where pneumocystis carinii pneumonia (a common fungus) was often the immediate cause of death and the Human Immunodeficiency Virus (HIV) is almost always listed as the underlying cause of death. However, HIV is not the pneumonia-causing pathogen which is the pneumocystis fungus. Instead, most pneumonia deaths, those included in the FluView numbers but not included in the leading causes of death numbers, were attributed to a cause such as a chronic lower respiratory disease, heart disease, cancer, even accidents, and other usually pre-existing conditions as the underlying cause of death.
The CDC follows the World Health Organization (WHO)’s definition of the underlying cause of death. WHO defines the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury” in accordance with the rules of the International Classification of Diseases (ICD).
In the United States, the underlying cause of death is listed last in the list of causes of death in part I of the death certificate. The immediate cause of death is listed first. Part 2 lists other conditions that are considered contributing factors but somehow not causes. Pneumonia is often the immediate cause of death in part 1 of the death certificate.
In principle, death certificates and the assignment of causes of death including the underlying cause of death is governed or at least guided by the CDC’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (2003 Revision). This one-hundred and thirty-eight (138) page manual actually provides very limited guidance on how to assign the underlying cause of death in cases where pneumonia is present. Page twenty-five (25) has the only detailed discussion of deaths involving pneumonia:
US CDC Medical Examiners’ Handbook 2003 suggests attributing a pneumonia death to either chronic ischemic heart disease or diabetes mellitus as the underlying cause but not the pneumonia or pneumonia-causingpathogen. No clear direction to the physician.
Pneumonia is often a nonspecific process that occurs as the terminal event in someone who dies of a more specific underlying cause of death, such as congestive heart failure resulting from ischemic heart disease. In such cases, the specific underlying cause of death should be included in the cause-of-death statement.
Pneumonia is often designated as either community acquired or hospital or institution acquired (nosocomial). If the community- or institution-acquired nature of the pneumonia is known, the cause-of-death statement should include an indication of which one applies.
The specific bacterial, viral, or other infectious agent, if known, should be cited in the cause-of-death statement.
Relevant risk factors should also be cited in the cause-of-death statement, as might occur in an alcoholic who develops tuberculous pneumonia. Only in those instances where pneumonia has caused death and there is no known underlying cause or risk factor should the underlying cause of death be stated as “Pneumonia,” being sure to specify the infectious agent, if known, or specifying that a specific etiology is unknown, if such is the case.
Emphasis Added
And on page 113 of Cause of Death and the Death Certificate by Randy Hanzlick, dementia, cerebrovascular disease, cardiac disease, and lung disease are all listed as common underlying causes of death in cases of deaths due to pneumonia:
Thus, traditionally, pre-2020 and COVID-19, pneumonia deaths were frequently assigned a non-pneumonia underlying cause of death, usually a pre-existing condition and not the pneumonia-causing pathogen such as the influenza virus or SARS-COV-2, in common medical practice. Based on the technical notes these pneumonia and influenza deaths would be included in the FluView death numbers but not in the leading causes of death report.
Comparing COVID-19 Death Numbers to the Pneumonia and Influenza Death Numbers and Estimates from Previous Years
As shown above, the CDC has at least three (3) different pneumonia and influenza death numbers and estimates: the Leading Causes of Death Report (about 55,000 deaths per year, about two percent of annual deaths from all causes), the FluView graph and underlying data from the NCHS (about 188,000 deaths per year, six to ten percent of annual deaths from all causes, before 2020), and the influenza death model estimates that range from 12,000 to 61,000 deaths per year with the best estimate close to the number of pneumonia and influenza deaths in the leading causes of death report. Are any of these the proper baseline for comparing COVID-19 deaths to prior years or should some other number or estimate be used?
In the absence of the RT-PCR and antibody tests for the SARS-COV-2 virus, most COVID-19 deaths would have been unexplained pneumonia deaths lacking a laboratory test confirming influenza or other known pathogen. Possibly, some COVID-19 deaths would have been listed as heart attacks or strokes, those COVID-19 deaths attributed to the blood clots and other blood-related anomalies currently blamed on COVID-19, or even some other causes. The rest of this article will focus on the pneumonia deaths which would probably comprise most of the COVID-19 deaths in the absence of laboratory tests.
The US CDC’s April 2020 guidelines for reporting COVID-19 deaths clearly direct physicians and others not to list chronic obstructive pulmonary disease (COPD) as the underlying cause of death in COVID-19 cases, moving it to Part 2 of the death certificate reserved for “non-cause” contributing factors, which differs dramatically from medical practice prior to 2020 as described in Randy Hanzlick’s book and implicit in the FluView pneumonia and influenza deaths data.
In some cases, survival from COVID–19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID–19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II and not in Part I.
This guidance also gives a specific example of a COVID-19 death with COPD relegated to Part 2:
COVID-19 Death Guidance Example with COPD as Contributing Factor Only
Although other causes of death that are often given as the underlying cause of death in pneumonia cases on pre-2020 death certificates are not explicitly identified in the April 2020 guidance document, it seems probable most physicians would move these pre-existing conditions to Part 2 and not list them as the underlying cause of death for COVID-19 based on the April 2020 CDC guidance document. Note that COPD would fall under the category “lung disease” in the list below from Randy Hanzlick’s Causes of Death and the Death Certificate:
Thus, COVID-19 deaths since the April 2020 guidance are probably roughly comparable to the FluView deaths, the larger number, the 188,000 pneumonia and influenza deaths per year. The language “roughly” is used because the April 2020 guidance appears to strongly encourage physicians and others to assign COVID-19 as the underlying cause of death in any death where COVID-19 is detected by tests or perhaps even just suspected, raising the possibility that heart attack and stroke deaths might be wrongly classified as COVID-19 deaths as well as the traditional pneumonia and influenza deaths that would be listed in the FluView data. These would presumably be misclassified as the COVID-19 deaths exhibiting the mysterious blood clots and other blood-related problems reported in some COVID-19 cases and deaths. Thus, the FluView death numbers may represent a lower bound on COVID-19 deaths rather than an exact baseline — unfortunately.
Ealy et al have raised the question whether the CDC complied with the Paperwork Reduction Act (PRA) and Information Quality Act (IQA) requirements in issuing the April and earlier March COVID-19 death certification guidelines, apparently without submitting these for public comment through the Federal Register as Ealy and co-authors claim is required by these federal laws.
Conclusion
Thus, due to the guidance on the death certificates from the CDC in April 2020, COVID-19 deaths on death certificates appear comparable to the larger FluView death numbers — or even larger numbers if heart attacks, strokes or other blood coagulation related deaths with a positive test or clinical diagnosis are being classified as COVID-19 deaths.
The CDC’s documents and web site are remarkably unclear, contradictory, and confusing for public health and scientific information presented to the general public, busy doctors and other medical professionals, or even research scientists — as previously noted by Peter Doshi and others.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).