Introduction
This is a summary (below) of our lengthy (about 13,000 word) paper on the many issues with the CDC’s pneumonia, influenza, and COVID-19 (PIC) death numbers. It is about 1,000 words in length (5-10 minute read) and summarizes most of our key findings.
John F. McGowan, Ph.D., Tam Hunt, Josh Mitteldorf, PhD. Improving CDC Data Practices Recommendations for Improving the United States Centers for Disease Control (CDC) Data Practices for Pneumonia, Influenza, and COVID-19 (v 1.1). Authorea. November 29, 2021. DOI:10.22541/au.163822197.79126460/v1
(https://doi.org/10.22541/au.163822197.79126460/v1)
URL:
https://www.authorea.com/users/425106/articles/547336-improving-cdc-data-practices-recommendations-for-improving-the-united-states-centers-for-disease-control-cdc-data-practices-for-pneumonia-influenza-and-covid-19-v-1-1
Key Points/Summary
A number of CDC data presentation and statistical practices since the start of the COVID-19 pandemic in early 2020 have not followed common scientific and engineering practice. Several problems with data presentation and analyses for pneumonia and influenza death numbers – which have been merged with COVID-19 death numbers in the FluView web site ‒ predate the pandemic.
Before the pandemic (March 2020), the non-standard data presentation and statistical practices appear to increase the number of deaths attributed to the influenza virus and imply the death counts are certain whereas substantial uncertainty exists due to uncertainty in the assignment of the cause of death and other reasons. Since the pandemic, these practices appear to do the same for SARS-COV-2 and COVID-19.
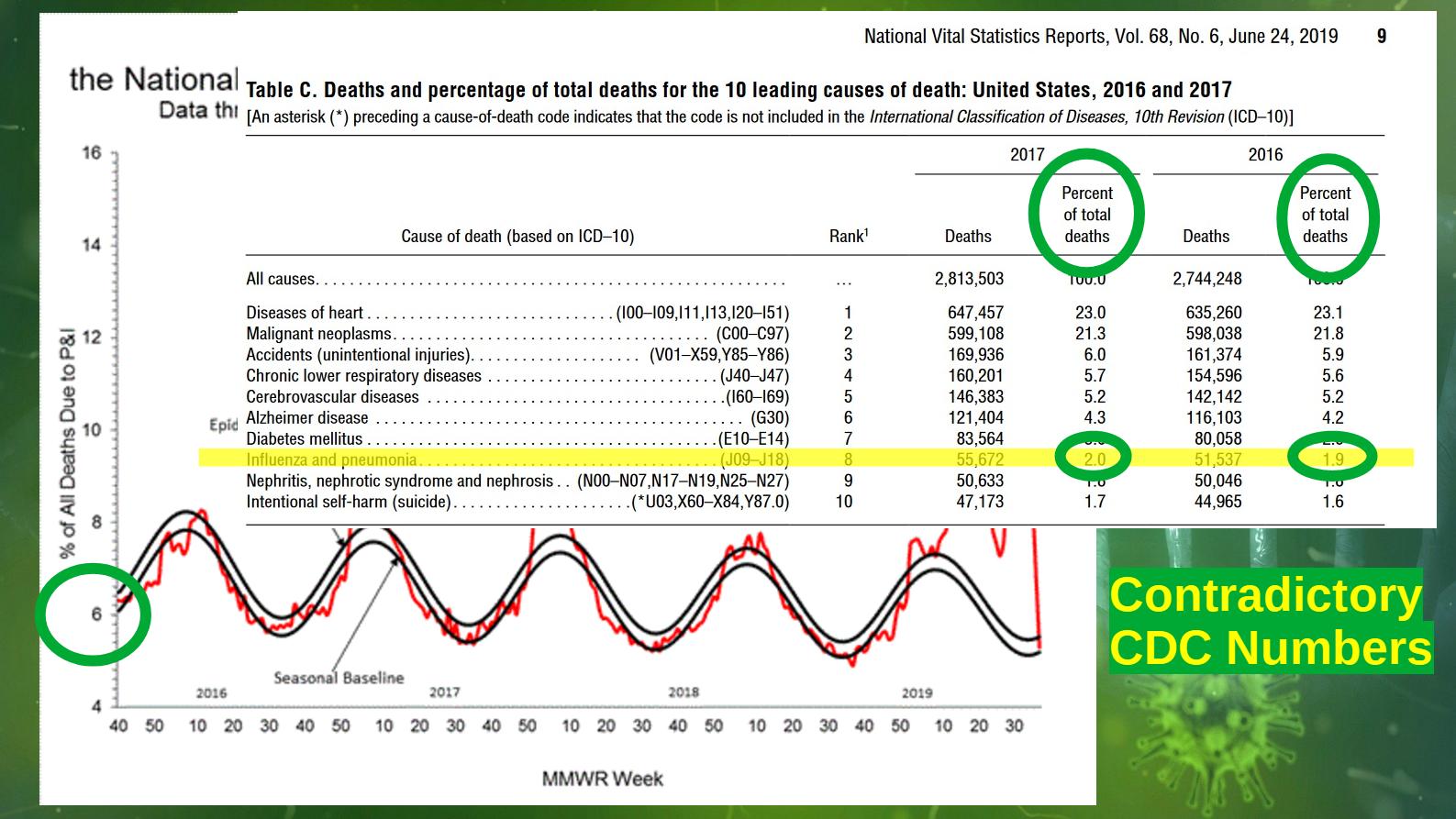
Remarkably, the CDC had at least three (3) different numbers for deaths attributed to pneumonia and influenza before 2020: the leading causes of death report count with about two (2) percent of deaths (about 55,000) per year attributed to influenza and pneumonia, the influenza virus deaths model with about 55,000 deaths per year attributed specifically to the influenza virus, and the FluView web site count with about 6-8 percent of deaths (about 188,000) per year attributed to pneumonia and influenza.
The FluView number differs from the other two death numbers by a factor of OVER THREE. The probable reason for this difference is that — according to the FluView technical notes — FluView counts deaths where pneumonia or influenza is listed as “a cause of death” whereas the leading cause of death report — according to the technical notes — counts only deaths where pneumonia or influenza is listed as “the underlying cause of death.” This probably reflects a large uncertainty in the assignment of the cause of death in respiratory illness cases; indeed the underlying cause of death may be ill-defined in many cases.
The CDC’s excess deaths estimates on their excess deaths web site does not report any standard goodness of fit statistics, notably the coefficient of determination often known as “R squared” and the “chi squared” goodness of fit statistic. Our analysis shows that different models with the same goodness of fit statistics give different estimates of the number of excess deaths, varying by up to 200,000 deaths in 2020. The CDC web site does not report this systematic modeling error.
The CDC appears to have chosen a set of parameters for the Noufaily/Farrington algorithm used to estimate excess deaths by the CDC that gives a lower “R Squared” value for goodness of fit than other choices and a HIGHER ESTIMATE of excess deaths — whereas common scientific and engineering practice would be to use the models with the best goodness of fit statistics, the “R Squared” closest to 1.0.
The Noufailly/Farrington algorithm is an empirical trend detection and extrapolation model theoretically incapable of accurately modeling the aging “baby boom” population which would be expected to produce “excess deaths” in recent years — nor is it able to explain the puzzling near stop of the increase in deaths per year reported in the immediate pre-pandemic years 2017-2019 despite the aging population.
The CDC does not publish (as of Dec 2021) years of life lost (YLL) estimates which include increases in suicides, homicides, and other adverse effects of the lockdowns, nor systematic modeling errors on the YLL estimates. YLL can illustrate the difference between a disease that largely kills those nearing death anyway versus a disease that easily kills the healthy.
The CDC issued a COVID death certificate guidance document in April of 2020 that appears to change the standards for assigning the underlying cause of death (UCOD) from the pre-pandemic practice for assigning the underlying cause of death for pneumonia and influenza, making COVID-19 the underlying cause of death in the many cases where the person who died had serious pre-existing conditions such as chronic bronchitis, emphysema, heart failure etc.. — the deaths counted in FluView but not in the leading causes of death report. There does not appear to have been any public comment on this guidance document to date.
In general the CDC does not report statistical errors, systematic errors, or estimates of biases in pneumonia, influenza, and COVID-19 death numbers. They do not report any monitoring of the effect of their guidance documents or other directives on the assignment of the cause of death by doctors, medical examiners, and others.
These issues are sometimes shared with other government agencies such as the US Social Security Administration (SSA) and US Census Bureau that work closely with the CDC.
Death counts for both individual causes and “all cause” deaths are frequently reported as precise to the last digit without any statistical or systematic errors, despite both known and unknown uncertainties in counting deaths, such as missing persons, unreported deaths due to deceased payee fraud, the ~1,000 living Americans incorrectly added to the government Deaths Master File (DMF), each month, for unknown reasons, and considerable uncertainties in assigning the underlying cause of death (UCOD) by coroners and doctors.
Similarly, raw counts, adjusted counts, and estimates – often based on incompletely documented computer mathematical models – are often not clearly identified as such. The Deaths Master File, with names and dates of death of deceased persons is exempt from the Freedom of Information Act (FOIA) and unavailable to the general public, independent researchers, and even other government agencies such as the IRS. This confidentiality of data makes independent verification of many CDC numbers, such as the excess deaths numbers tracked during the COVID-19 pandemic, all but impossible.
This omission of common scientific and engineering practices raises questions about the accuracy of the CDC’s data, conclusions, and public health policies in a number of important areas, including the COVID-19 pandemic.
The non-standard data presentation and statistical practices appear to increase the number of deaths attributed to the influenza virus and imply the death counts are certain whereas substantial uncertainty exists due to uncertainty in the assignment of the cause of death and other causes. Since the pandemic, these practices appear to do the same for SARS-COV-2 and COVID-19.
END OF SUMMARY
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).