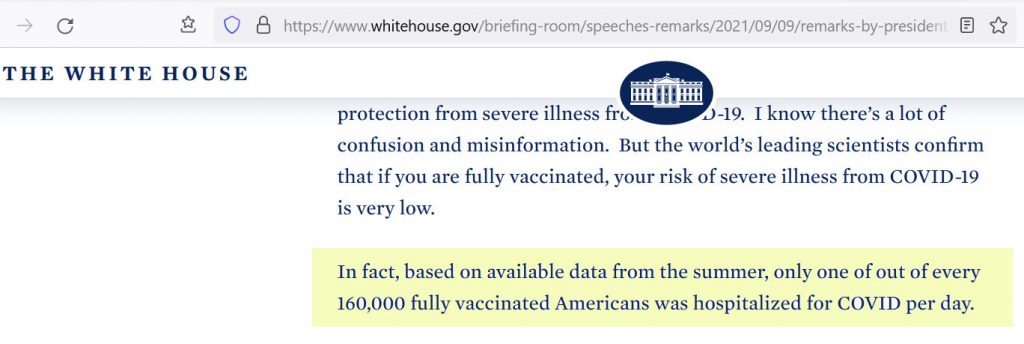
In fact, based on available data from the summer, only one of out of every 160,000 fully vaccinated Americans was hospitalized for COVID per day.
This actually means that over 1,000 fully vaccinated American per day were hospitalized, around 90,000 over the three months of summer if this refers to new hospitalizations per day rather than number of people in a hospital on each day, suggesting around 4-9 million fully vaccinated Americans were infected with the virus during the summer when respiratory viruses are at a seasonal low.
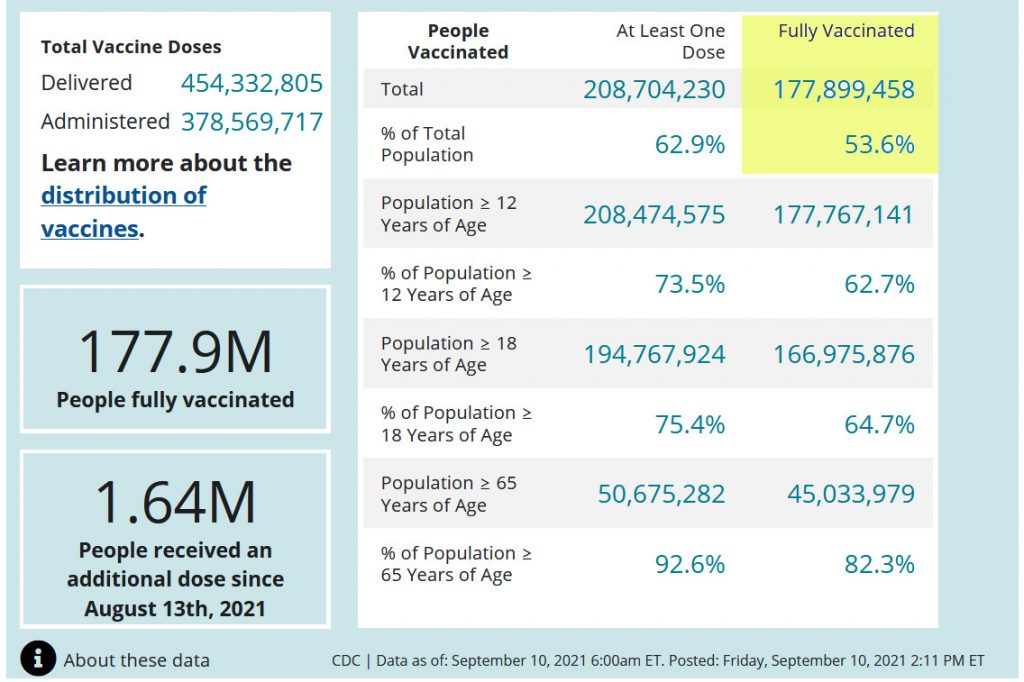
The US federal government currently (Sep 10, 2021) claims about 53 percent of American are fully vaccinated. There are about 330 million people in the United States. This means about 175 million Americans are fully vaccinated. If one (1) in 160,000 fully vaccinated Americans was hospitalized for COVID per day, this works out to (175 million/160,000) about 1,093 American hospitalized per day.
COVID has an infection fatality rate (IFR) of around 0.3 percent (not the case fatality rate or CFR which is often confused with the IFR, which is usually the fractions of deaths among symptomatic cases reported by doctors or hospitals — not people who stay home and recover or simply have no or negligible symptoms). Probably a few percent of people infected with COVID actually are hospitalized.
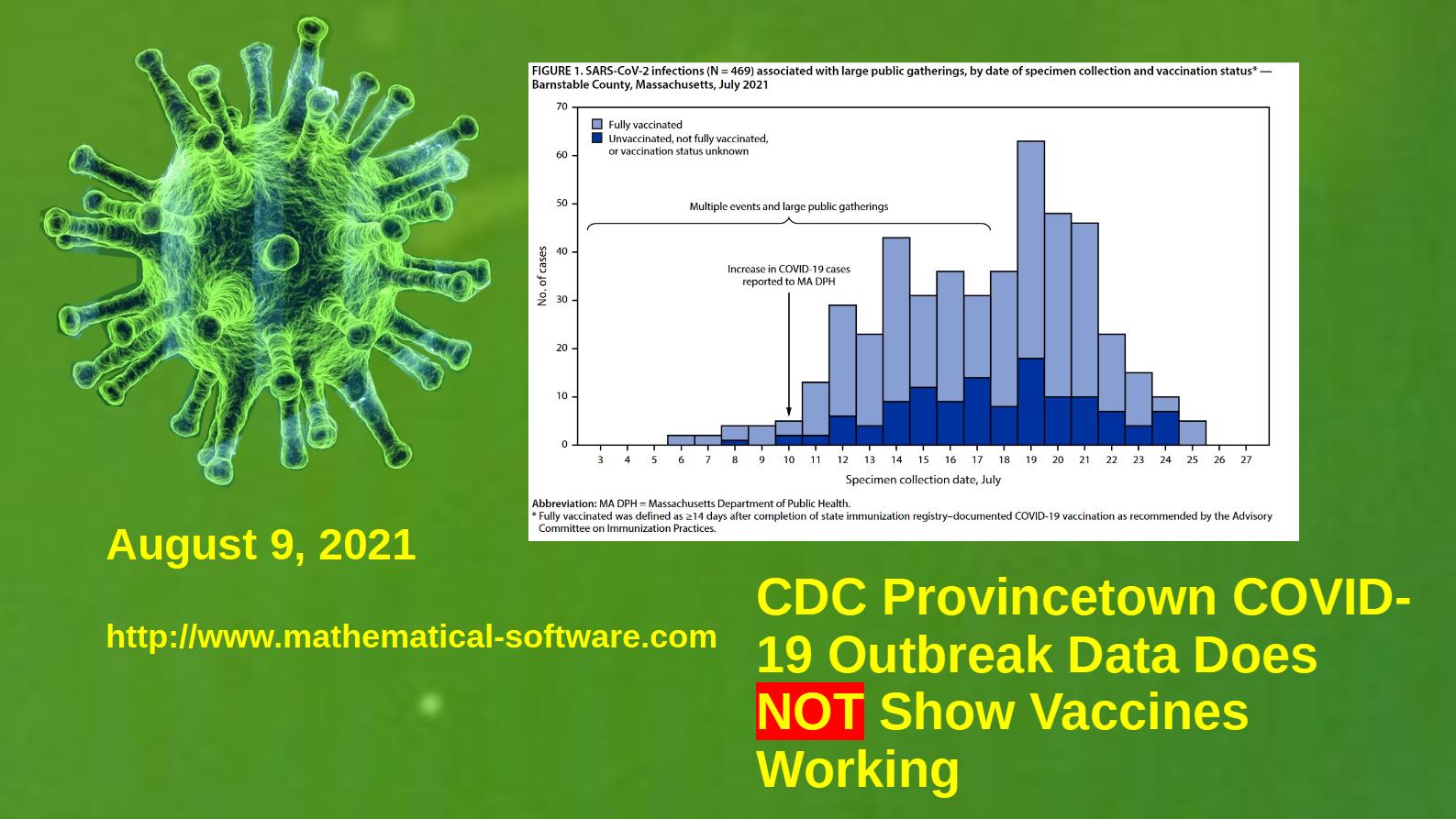
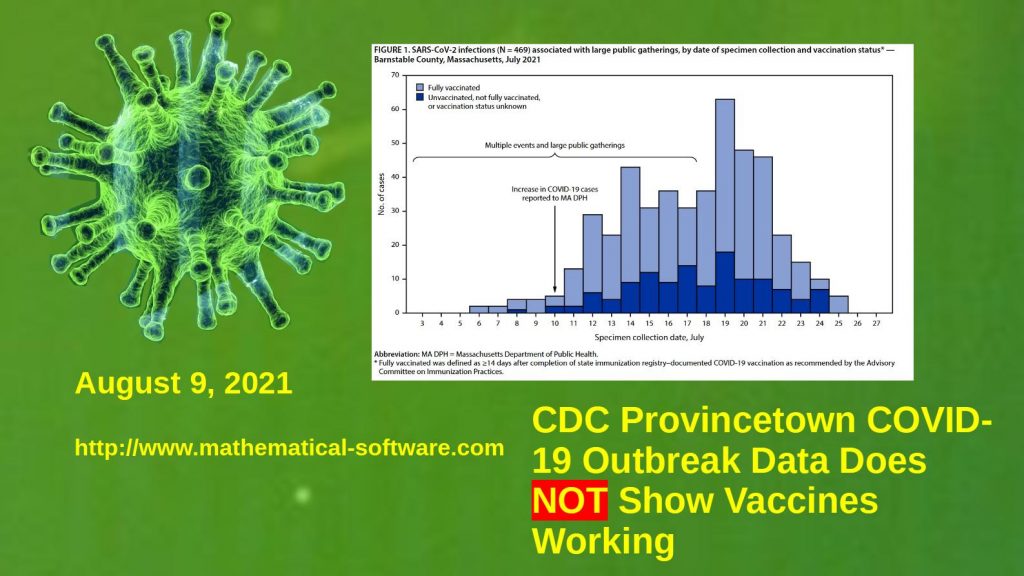
For example in the recent Provincetown, Cape Cod (Barnstable County, Massachusetts) outbreak four (4) fully vaccinated people out of 346 fully vaccinated persons identified by the CDC and Massachusetts state public health contact tracing were hospitalized, giving a hospitalization rate of about (4/346) 1.16 percent of the fully vaccinated. The hospitalization rate for the unvaccinated in the Provincetown outbreak was statistically the same as the hospitalization rate for the fully vaccinated — about one (1) percent.
Using a one percent hospitalization rate among the fully vaccinated means that nine (9) million fully vaccinated American were infected with COVID-19 during the summer of 2021, despite the vaccines and the seasonal low in respiratory viral diseases. A more conservative hospitalization rate of two (2) percent gives 4.5 million Americans infected.
Even if President Biden’s number refers to the number of fully vaccinated persons in a hospital each day rather than new hospital admissions with COVID, assuming a typical stay of two weeks in a hospital with COVID, this gives about 6,000 hospitalizations over a three month (six two-week periods) summer, meaning 300,000 to 600,000 fully vaccinated persons infected with COVID during the seasonal summer low in respiratory viral diseases.
What Does This Mean?
As with the official CDC report on the Provincetown, Cape Cod, Massachusetts outbreak and disappointing result in Israel, President Biden’s highly misleading number strongly suggests the COVID vaccines are failing to prevent infection by COVID and the spread of the disease on a large scale.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The Provincetown, Massachusetts (Cape Cod, Barnstable County) COVID-19 outbreak does NOT prove that the COVID-19 vaccines are working as widely claimed in the mainstream media. (See the CDC Report “Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings — Barnstable County, Massachusetts,” https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf)
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This is a preprint of a new academic paper written by Tam Hunt, Josh Mitteldorf, Ph.D. and myself on the US Centers for Disease Control (CDC)’s data practices during the COVID-19 pandemic and for pneumonia and influenza prior to the pandemic. I am the corresponding author.
Abstract
During the pandemic, millions of Americans have become acquainted with the CDC because its reports and the data it collects affect their day-today lives. But the methodology used and even some of the data collected by CDC remain opaque to the public and to the community of academic epidemiology. In this paper, we highlight areas in which CDC methodology might be improved and where greater transparency might lead to broad collaboration. (1) “Excess” deaths are routinely reported, but not “years of life lost”, an easily-computed datum that is important for public policy. (2) What counts as an “excess death”? The method for computing the number of excess deaths does not include error bars and we show a substantial range of estimates is possible. (3) Pneumonia and influenza death data on different CDC pages is grossly contradictory. (4) The methodology for computing influenza deaths is not described in sufficient detail that an outside analyst might pursue the source of the discrepancy. (5) Guidelines for filling out death certificates have changed during the COVID-19 pandemic, preventing the comparison of 2020-21 death profiles with any previous year. We conclude with a series of explicit recommendations for greater consistency and transparency, and ultimately to make CDC data more useful to outside epidemiologists.
John F. McGowan, Ph.D., Tam Hunt, Josh Mitteldorf. Improving CDC Data Practices Recommendations for Improving the United States Centers for Disease Control (CDC) Data Practices for Pneumonia, Influenza, and COVID-19. Authorea. July 19, 2021. DOI: 10.22541/au.162671168.86830026/v1
Here are the key recommendations from the paper:
Recommendations
In light of the previous discussion, we make a number of recommendations to improve CDC’s data practices, including improved observance of common scientific and engineering practice – such as use of significant figures and reporting of statistical and systematic errors. Common scientific and engineering practice is designed to prevent serious errors and should be followed rigorously in a crisis such as the COVID-19 pandemic.
Note that some of these recommendations may require changes in federal or state laws, federal or state regulations, or renegotiation of contracts between the federal government and states. This is probably the case for making the Deaths Master File (DMF), with names and dates of death of persons reported as deceased to the states and federal government, freely available to the public and other government agencies.
All CDC numbers, where possible, should be clearly identified as estimates, adjusted counts, or raw counts, with statistical errors and systematic errors given, using consistent clear standard language in all documents. The errors should be provided as both ninety-five percent (95%) confidence level intervals and the standard deviation – at least for the statistical errors.
In the case of adjusted counts, the raw count should be explicitly listed immediately following the adjusted count as well as a brief description of the adjustment and a reference for the adjustment methodology. For example, if the adjusted number of deaths in the United States in 2020 is 3.4 million but the raw count of deaths was 3.3 million with 100,000 deaths added to adjust for unreported deaths of undocumented immigrants, the web pages and reports would say:
Total deaths (2020): 3.4 million (adjusted, raw count 3.3 million, unreported deaths of undocumented immigrants, adjustment methodology citation: Smith et al, MMWR Volume X, Number Y)
The distinction between the leading causes of death report “pneumonia and influenza” deaths, ~55,000 per year pre-pandemic, and the FluView website “pneumonia and influenza” deaths, ~188,000 per year pre-pandemic, should be clarified in the labels and legends for the graphics and prominently in the table of leading causes of death or immediately adjacent text. Statistical and systematic errors on these numbers should be provided in graphs and tables.
In general, where grossly different raw counts, adjusted counts, or estimates are presented in CDC documents and websites with the same name, semantically equivalent or nearly equivalent names such as “pneumonia and influenza” and “influenza and pneumonia,” clearly distinct names should be used instead, or the reasons for the gross difference in the values should be prominently listed in the graphs and tables or immediately adjacent text. It should be easy for the public, busy health professionals, policy makers and others to recognize and understand the differences.
CDC should provide results for different models for the same data with similar R2 values – coefficient of determination – to give the audience a quick sense of the systematic modeling errors – since there is no generally accepted methodology for estimating the 95% confidence level for the systematic modeling errors. See Figure 7 above for an example.
All mathematical models should be free and open source with associated data provided using commonly used free open-source scientific programming languages such as Python or R, made available on the CDC website, GitHub, and other popular sources. The models and data should be provided in a package form such that anyone with access to a standard MS Windows, Mac OS X, or Linux/Unix computer can easily download and run the analysis – similar to the package structure used by the GNU project, for example.
Specifically, the influenza virus deaths model should be provided to the public as code and data. The justification for the increase in the number of deaths attributed to influenza (~6,000 to ~55,000) should be presented in clear language with supporting numbers, such as the false positive and negative rates for the laboratory influenza deaths and general diagnosis of influenza in the absence of a positive lab test as well as in the code and data.
With respect to excess deaths tracking, include all major select causes of death, rather than just the thirteen (13) in the cause-specific excess deaths that CDC tracks, which currently account for about 2/3 of all deaths.
Include a Years of Lives Lost (YLL) display for COVID-19 deathsi and non-COVID-19 deaths, as well as excess deaths analysis, due to the higher granularity of YLL analysis when compared to excess deaths analysis. Explain the pros and cons of both analytical tools. Do the same for any future pandemics or health crises.
Adopt or develop a different algorithm or algorithms for tracking excess deaths which are mostly attributed to non-infectious causes such as heart attacks, cancer, and strokes. The Farrington/Noufaily algorithms were specifically developed as an early warning for often non-lethal infectious disease outbreaks such as salmonella. A medically-based model or models that incorporates population demographics such as the aging “baby boom” and evolving death rates broken down by age, sex, and possibly other factors where known is probably a better practice rather than simple empirical trend models such as the Noufaily algorithm.
Eliminate the zeroing procedure in calculating excess deaths, in which negative excess deaths in some categories are set to zero, rather than being added to the full excess deaths sum over all categories.
The anonymized data with causes of death as close to the actual data as possible, e.g. the actual death certificates, should be available on the CDC website in a simple accessible widely used format such as CSV (comma separated values) files. The code used to aggregate the data into summary data such as the FluView website data files should also be public.
The full Deaths Master File (DMF) including the actual names of the deceased persons and dates of death should be made available to the general public, independent researchers, and others. This is critical to independent verification of many numbers from the CDC, SSA, and US Census.
COVID-19-related deaths figures should be tracked based on year-specific age of death, rather than 10-year age ranges, as is currently the case.
CDC frequently changes the structure and layout of the CSV files/spreadsheets on their websites. The CDC should either (1) not do this or (2) provide easy conversion between different file formats with each new format so it is trivial for third parties to quickly adapt to the changes without writing additional code. CDC should provide a program or program in a free and open source language like R to convert between the formats.
The CDC and other agencies should be required to announce and solicit public comment for changes to case definitions, data collection rules, etc. for key public policy data such as the COVID-19 case definitions, death certification guidelines, and coding rules. Other government agencies have significantly more public participation than CDC, which is appropriate in a modern democracy.
Any practices and policies imposed in a public emergency, such as case definitions, definitions of measured quantities, data reporting practices, etc. imposed without public comment and review, should have an expiration date (e.g. sixty days) beyond which they must be subject to public review. Public comment, reviews, and cost/benefit analyses should happen during this emergency period.
Enacting these reforms should reduce the risk of serious errors, increase the quality and accuracy of CDC data and analyses, as well as any policies or CDC guidelines based on the data and analysis, and strengthen public confidence in the CDC and public health policies.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
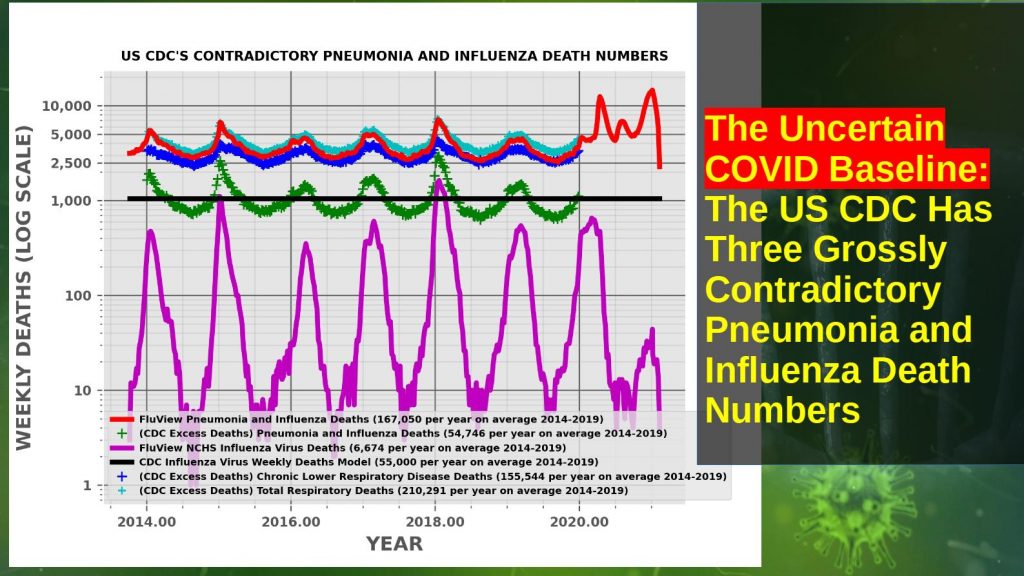
US CDC’s Contradictory Pneumonia and Influenza Weekly Death Numbers 2014-2019
The United States Centers for Disease Control (CDC) has at least three different, grossly contradictory historical pneumonia and influenza death numbers. The CDC FluView pneumonia and influenza pre-COVID death number is OVER THREE TIMES the leading causes of death number. Pneumonia and influenza are often conflated in the CDC’s documentation and in the CDC’s influenza death model.
These death numbers are frequently used as the baseline for comparison of the COVID-19 death numbers and assessing the severity of the pandemic relative to previous years and pandemics such as the 1957, 1968, and 2009 influenza pandemics.
The Three Different Sets of Pneumonia and Influenza Death Numbers
Leading Causes of Death Pneumonia and Influenza (P&I) Deaths (About 55,000 per year)
FluView Pneumonia and Influenza (P&I) Deaths (About 167,000 pre-COVID, Over THREE TIMES Leading Causes of Death, About 7,000 Influenza Virus Deaths Per Year)
CDC Model Influenza Virus Deaths (About 55,000 per year, at least THREE TIMES FluView Influenza Deaths)
This is the program and data files used to generate the plot above comparing the CDC’s pneumonia and influenza death numbers from 2014 through 2019. Download and use the 7-Zip or other file archiver for MS Windows or the Unix command tar -xvf cdc_numbers.tar to unpack the program and data files.
This Python 3 program generates a plot comparing the different numbers on a log scale for easy comparison.
The program also plots the weekly deaths for “chronic lower respiratory disease,” mostly chronic bronchitis and emphysema — also referred to as “chronic obstructive pulmonary disease” in the medical literature. It is likely that the THREE TIMES LARGER FluView pneumonia and influenza death numbers are produced by borrowing deaths from chronic lower respiratory disease (mostly chronic bronchitis and emphysema) and adding them to the “pneumonia and influenza” deaths reported in the leading causes of death report.
discusses these issues in much more detail and provides references and links.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This article argues that the US Centers for Disease Control (CDC)’s April 2020 guidance for filling out death certificates for possible COVID-19 related deaths strongly encourages, if not requires, assigning COVID-19 as the underlying cause of death (UCOD) in any death where COVID-19 or the SARS-COV-2 virus may be present, which appears to differ from common historical practice for pneumonia and influenza deaths where pneumonia was frequently treated as a “complication,” a cause of death but not the underlying cause of death.
This means the number of COVID deaths should be compared to a count of death certificates where pneumonia and influenza were listed as a cause of death or even a lesser contributing factor, a historical number which appears to have been at least 188,000 per year based on the CDC FluView web site. The proper comparison number may be even larger if deaths that historically were listed as heart attacks, cancer or other causes than pneumonia or influenza are also being reassigned due to the April 2020 guidance.
The CDC has at least three different historical pneumonia and influenza death numbers. These are the leading causes of death report numbers of about 55,000 deaths per year which appears based on death certificates, a poorly documented mathematical/computer model which attributes about 55,000 deaths per year with a large error to the influenza virus, and the FluView web site which attributed about 188,000 deaths per year to pneumonia and influenza.
The leading causes of death historical numbers appear based on the underlying cause of death listed on the death certificate whereas the FluView historical numbers appear based on death certificates that list pneumonia or influenza as a cause of death, in most cases not the underlying cause of death. The historical FluView death numbers appear to be the proper baseline for comparison to COVID-19, although an even larger number is possible if there has been practically significant reassignment of heart attacks and other deaths as well.
This would mean that COVID-19 is less deadly than popular perceptions based frequently on comparisons to “flu death numbers” of about 55,000 per year apparently derived either from the CDC’s leading causes of death report or the influenza virus model.
Note that this is not a claim that COVID-19 or SARS-COV-2 plays no causal role in the deaths: a death “with” COVID rather than a death “due to” COVID in popular debates. Rather, the proper interpretation is probably that COVID-19 acts predominantly as an opportunistic infection instead of an inherently deadly infection able to easily kill healthy young people with a strong immune system. Vaccines are likely to have small or no ability to prevent death from an opportunistic infection since the infected vaccinated person will have a weak or failed immune system with little or no ability to produce the immune response learned from the vaccination.
The language and numbers on the CDC web sites and official reports and documents are remarkably confusing and grossly contradictory in some cases — such as the historical number of deaths attributed to pneumonia and influenza which differs by over a factor of THREE. Error bars or confidence levels on most numbers such as the death numbers are not reported as required by common scientific and engineering practice. These practices have been harshly criticized for years by scientists and medical experts such as Peter Doshi. Consequently it is impossible to make definite statements about the meaning of the numbers and the definitions of measured quantities discussed below.
This is a complex life-and-death subject with many nuances. Each section below expands each key point in detail, discussing the nuances and unknowns. Some facts and arguments are repeated in different sections for clarity.
Three Different Historical Pneumonia and Influenza Death Numbers
The United States Centers for Disease Control (CDC) documents and web site present at least THREE different historical (pre-2020) estimates of deaths from “influenza and pneumonia,” “pneumonia and influenza,” and/or “influenza” or the “flu” presumably meaning the influenza category of viruses. Which of these three death numbers, one of which differs by a factor of OVER THREE from the other two, should be compared to COVID-19 deaths? Indeed, it could well be incorrect to compare any of them to the COVID-19 deaths.
These three pneumonia and influenza death numbers are the value in the annual leading causes of death report — about 55,000 deaths each year, the tables of “pneumonia and influenza” (abbreviated as P&I) from the National Center for Health Statistics (NCSH) used on the FluView web site — about 188,000 deaths per year, OVER THREE TIMES the leading causes of death number, and the output of a poorly documented model of deaths attributed to the influenza category of viruses, a broad range centered at about 55,000 deaths per year.
Deaths attributed to COVID-19 in 2020 have frequently been compared to an estimate of about 55,000, either to the date of the report or for the entire year. The language used is often unclear but appears to refer to either the CDC’s influenza mathematical model or the leading causes of death number, which are similar numbers but technically not the same.
This article argues that the current COVID-19 death numbers are best compared to the larger FluView numbers, although an even larger different number may be appropriate if deaths that would have been attributed to heart attacks, strokes, or other blood coagulation related disorders in the absence of a positive SARS-COV-2 test or diagnosis are included in the current COVID-19 death counts.
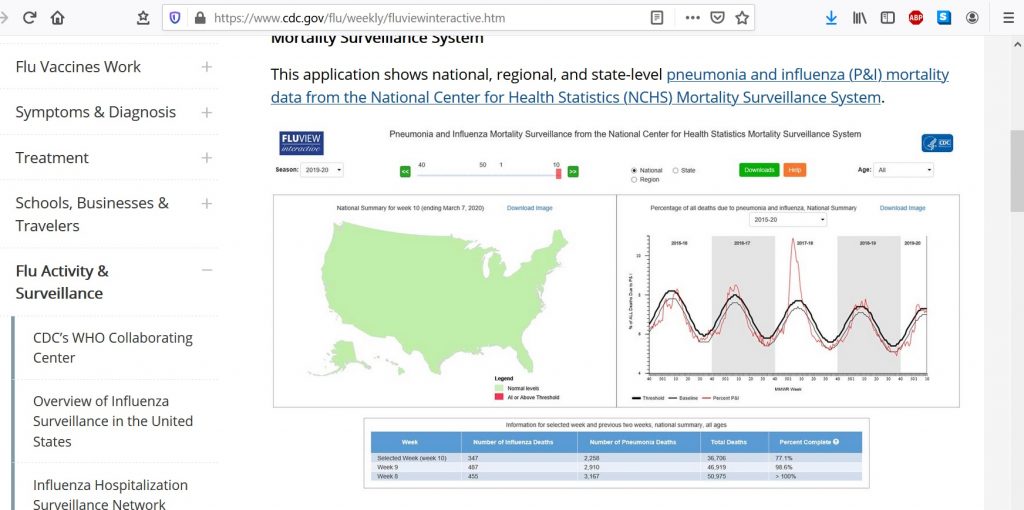
The CDC FluView Web Site
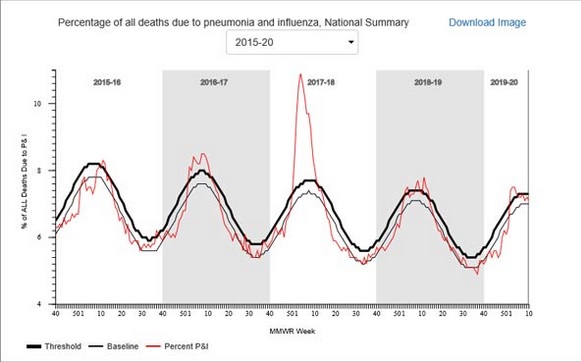
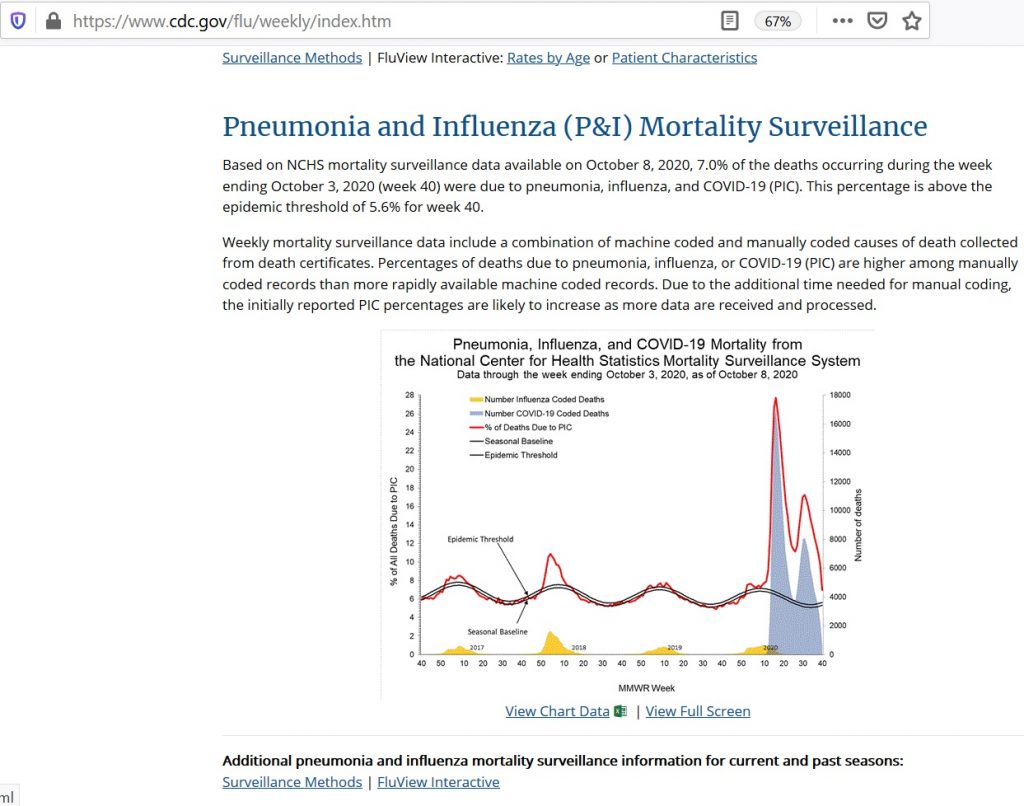
The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluViewPneumonia & Influenza Mortality plot. The underlying data files from the National Center for Health Statistics (NCHS) list about 188,000 deaths per year attributed to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
Note also that deaths attributed to “pneumonia and influenza” on the FluView web site are highly seasonal. A substantial increase over the summer is expected during the winter (or rainy season in Northern California and similar regions), peaking in December and January each year.
Also note that the seasonal variation is sinusoidal — like the oscillation of a pendulum or a mechanical spring. Contrary to popular culture, there is no clear step up when schools open in the fall or step down when schools close for the summer. It looks very much like something driven by the Sun, directly or indirectly by some mechanism or mechanisms. Possible mechanisms include Vitamin D production from sunlight, destruction of viruses and bacteria in the air or on surfaces by ultraviolet light in sunlight, general health benefits of a warm environment, or some other Sun-driven phenomenon.
The Leading Causes of Death Report
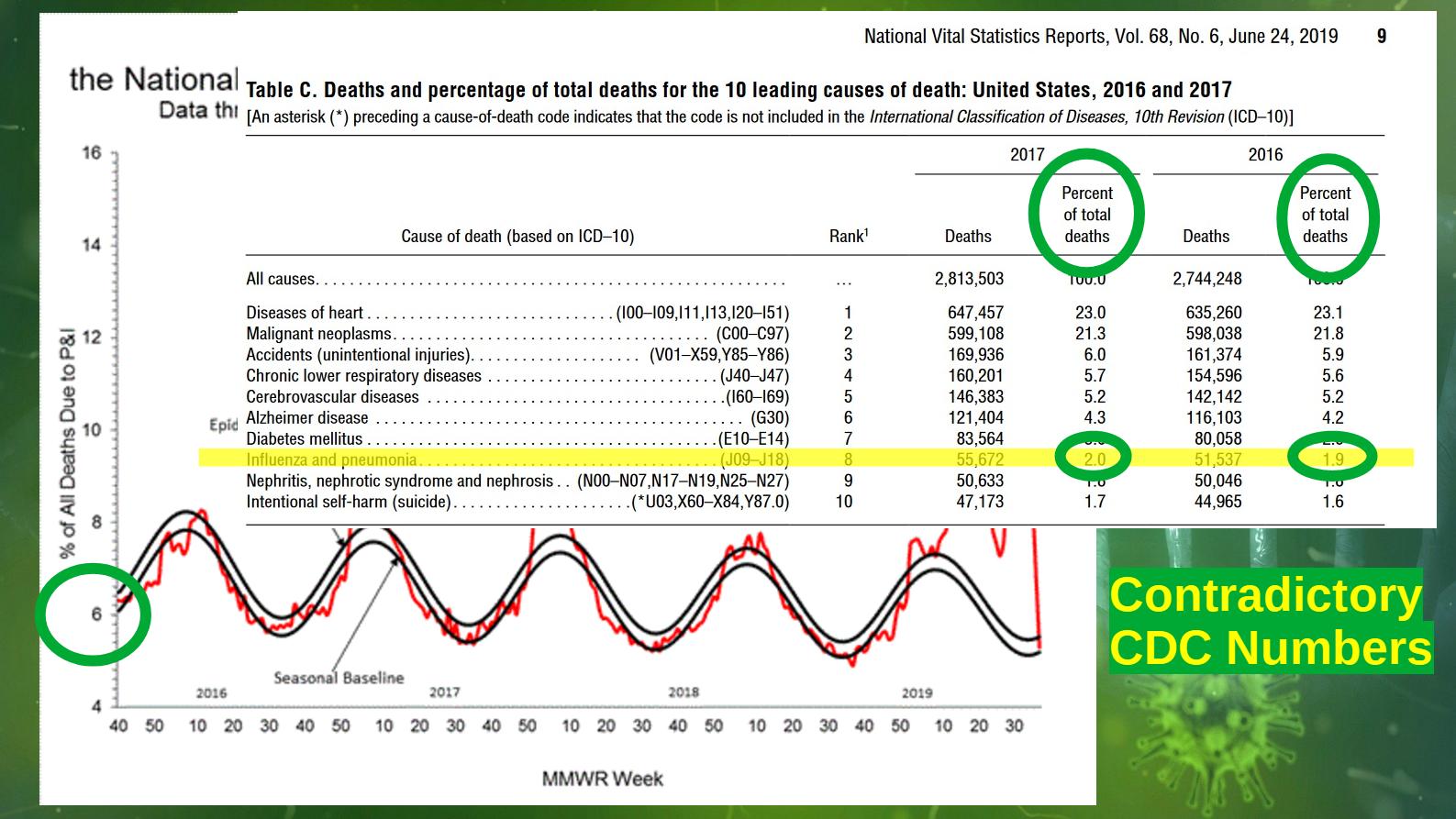
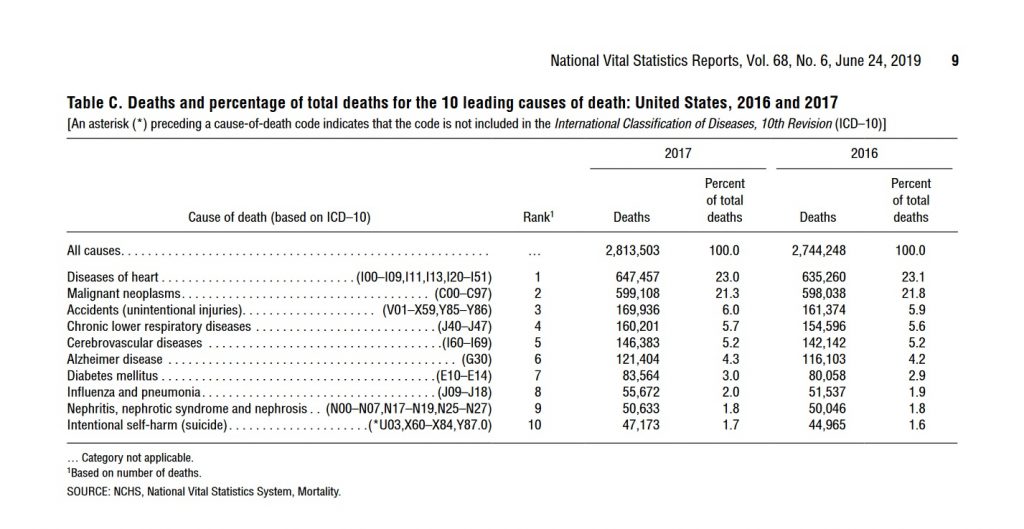
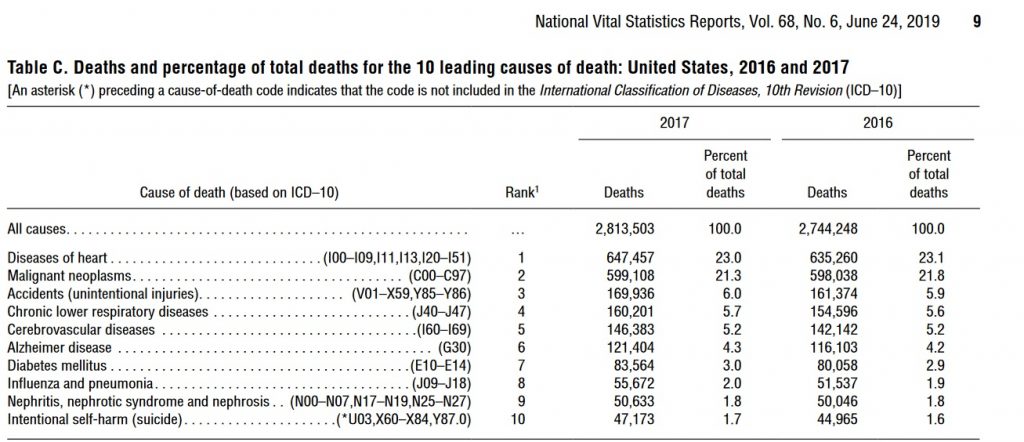
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.”
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
A longer, more detailed discussion of the FluView, leading causes of death, and the CDC’s influenza virus death model death numbers (yet another number) may be found below. It appears likely the FluView death numbers are defined similarly to current COVID-19 death counts; the reasons for this are explained in some detail.
Which Pneumonia and Influenza Death Numbers Should Be Compared to the COVID-19 Death Numbers?
The FluView and Leading Causes of Death numbers for “pneumonia and influenza” differ by a factor of OVER THREE. Note that both the FluView and Leading Causes of Death numbers have no error bars or error estimates given, implying exact numbers in common scientific and engineering practice. Should the number of COVID-19 deaths be compared to the FluView number or the leading causes of death number or some other number?
The CDC also uses a poorly documented mathematical model that attributes roughly 55,000 deaths from pneumonia and influenza to the influenza virus as the underlying cause, a number roughly comparable to the total pneumonia and influenza deaths in the leading causes of death. The influenza virus is confirmed by laboratory tests in only a small fraction of pneumonia and influenza deaths, about 6,000 per year.
Although the language is often unclear in the CDC documents and web site, the CDC appears to claim that an initial influenza infection which disappears or becomes undetectable in laboratory tests leads to the subsequent pneumonia, presumably a bacterial pneumonia although other viruses would be consistent with some lab tests. Based on this argument, the CDC appears to attribute most pneumonia deaths where historically pneumonia was listed as the “underlying cause of death” to the influenza virus for which there is a flu vaccine that the CDC promotes heavily — even though laboratory tests frequently fail to confirm influenza or even detect other viruses or bacteria instead. The “underlying cause of death” is discussed in more detail below.
As shown in the graphic above, the CDC web site Disease Burden of Influenza (Figure 1) appears to give a range from 12,000 to 61,000 influenza deaths from this model. The graphic does not indicate if this range is a 95 percent confidence interval — a common scientific and engineering practice — or some other error estimate. The range in the graphic does not appear to match any of the 95 percent confidence levels for estimated deaths attributed to influenza in Table 1.
The History of Serious Criticism of the CDC’s “Flu” Death Numbers
There is a long history of serious criticism of the CDC’s “flu” death numbers by medical scientists and others. The most prominent critic is Peter Doshi, currently a professor at the University of Maryland and an associate editor at the British Medical Journal.
Citing the results of actual laboratory tests of deceased patients, critics of the CDC’s flu death numbers such as University of Maryland Professor Peter Doshi have argued that pneumonia deaths are due to a range of different viruses, bacteria, other pathogens, and even toxins, rather than predominantly influenza as implied by the CDC’s influenza deaths model. The output of this model appears to be the basis of the baseline “flu” deaths numbers used in most popular and public policy discussions of COVID-19 deaths — although the leading causes of death report number may also be used.
The Reason for the Large Difference Between the FluView and Leading Causes of Death Numbers
The US CDC documents and web site are frequently unclear and even contradictory as in the case of these grossly contradictory totals of deaths from pneumonia and influenza. This makes it difficult to be certain of the cause for the difference. Nonetheless, the technical notes for each document — FluView and the leading causes of death — give a highly probable reason.
Leading Causes of Death Report for 2017 with “the underlying cause of death” language circled in red. (Dec. 18, 2020)
Death certificates frequently have multiple causes of death. One of these is assigned as the underlying cause of death. This may be quite arbitrary in some cases. Indeed the concept of “underlying cause of death” may not be well defined for some deaths because the aged may develop multiple health problems in parallel that are fatal in combination.
FluView Mortality Surveillance notes with “A Cause of Death” Language Circled in Red (Dec. 18, 2020)
The Rules for Assigning the Underlying Cause of Death Before COVID-19
Prior to 2020 and COVID-19, most pneumonia deaths did not list pneumonia or the pneumonia-causing pathogen if known as the underlying cause of death. This will be discussed in detail below. The only common partial exception was HIV/AIDS where pneumocystis carinii pneumonia (a common fungus) was often the immediate cause of death and the Human Immunodeficiency Virus (HIV) is almost always listed as the underlying cause of death. However, HIV is not the pneumonia-causing pathogen which is the pneumocystis fungus. Instead, most pneumonia deaths, those included in the FluView numbers but not included in the leading causes of death numbers, were attributed to a cause such as a chronic lower respiratory disease, heart disease, cancer, even accidents, and other usually pre-existing conditions as the underlying cause of death.
The CDC follows the World Health Organization (WHO)’s definition of the underlying cause of death. WHO defines the underlying cause of death as “the disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury” in accordance with the rules of the International Classification of Diseases (ICD).
In the United States, the underlying cause of death is listed last in the list of causes of death in part I of the death certificate. The immediate cause of death is listed first. Part 2 lists other conditions that are considered contributing factors but somehow not causes. Pneumonia is often the immediate cause of death in part 1 of the death certificate.
In principle, death certificates and the assignment of causes of death including the underlying cause of death is governed or at least guided by the CDC’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (2003 Revision). This one-hundred and thirty-eight (138) page manual actually provides very limited guidance on how to assign the underlying cause of death in cases where pneumonia is present. Page twenty-five (25) has the only detailed discussion of deaths involving pneumonia:
US CDC Medical Examiners’ Handbook 2003 suggests attributing a pneumonia death to either chronic ischemic heart disease or diabetes mellitus as the underlying cause but not the pneumonia or pneumonia-causingpathogen. No clear direction to the physician.
Pneumonia is often a nonspecific process that occurs as the terminal event in someone who dies of a more specific underlying cause of death, such as congestive heart failure resulting from ischemic heart disease. In such cases, the specific underlying cause of death should be included in the cause-of-death statement.
Pneumonia is often designated as either community acquired or hospital or institution acquired (nosocomial). If the community- or institution-acquired nature of the pneumonia is known, the cause-of-death statement should include an indication of which one applies.
The specific bacterial, viral, or other infectious agent, if known, should be cited in the cause-of-death statement.
Relevant risk factors should also be cited in the cause-of-death statement, as might occur in an alcoholic who develops tuberculous pneumonia. Only in those instances where pneumonia has caused death and there is no known underlying cause or risk factor should the underlying cause of death be stated as “Pneumonia,” being sure to specify the infectious agent, if known, or specifying that a specific etiology is unknown, if such is the case.
Emphasis Added
And on page 113 of Cause of Death and the Death Certificate by Randy Hanzlick, dementia, cerebrovascular disease, cardiac disease, and lung disease are all listed as common underlying causes of death in cases of deaths due to pneumonia:
Thus, traditionally, pre-2020 and COVID-19, pneumonia deaths were frequently assigned a non-pneumonia underlying cause of death, usually a pre-existing condition and not the pneumonia-causing pathogen such as the influenza virus or SARS-COV-2, in common medical practice. Based on the technical notes these pneumonia and influenza deaths would be included in the FluView death numbers but not in the leading causes of death report.
Comparing COVID-19 Death Numbers to the Pneumonia and Influenza Death Numbers and Estimates from Previous Years
As shown above, the CDC has at least three (3) different pneumonia and influenza death numbers and estimates: the Leading Causes of Death Report (about 55,000 deaths per year, about two percent of annual deaths from all causes), the FluView graph and underlying data from the NCHS (about 188,000 deaths per year, six to ten percent of annual deaths from all causes, before 2020), and the influenza death model estimates that range from 12,000 to 61,000 deaths per year with the best estimate close to the number of pneumonia and influenza deaths in the leading causes of death report. Are any of these the proper baseline for comparing COVID-19 deaths to prior years or should some other number or estimate be used?
In the absence of the RT-PCR and antibody tests for the SARS-COV-2 virus, most COVID-19 deaths would have been unexplained pneumonia deaths lacking a laboratory test confirming influenza or other known pathogen. Possibly, some COVID-19 deaths would have been listed as heart attacks or strokes, those COVID-19 deaths attributed to the blood clots and other blood-related anomalies currently blamed on COVID-19, or even some other causes. The rest of this article will focus on the pneumonia deaths which would probably comprise most of the COVID-19 deaths in the absence of laboratory tests.
The US CDC’s April 2020 guidelines for reporting COVID-19 deaths clearly direct physicians and others not to list chronic obstructive pulmonary disease (COPD) as the underlying cause of death in COVID-19 cases, moving it to Part 2 of the death certificate reserved for “non-cause” contributing factors, which differs dramatically from medical practice prior to 2020 as described in Randy Hanzlick’s book and implicit in the FluView pneumonia and influenza deaths data.
In some cases, survival from COVID–19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID–19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II and not in Part I.
This guidance also gives a specific example of a COVID-19 death with COPD relegated to Part 2:
COVID-19 Death Guidance Example with COPD as Contributing Factor Only
Although other causes of death that are often given as the underlying cause of death in pneumonia cases on pre-2020 death certificates are not explicitly identified in the April 2020 guidance document, it seems probable most physicians would move these pre-existing conditions to Part 2 and not list them as the underlying cause of death for COVID-19 based on the April 2020 CDC guidance document. Note that COPD would fall under the category “lung disease” in the list below from Randy Hanzlick’s Causes of Death and the Death Certificate:
Thus, COVID-19 deaths since the April 2020 guidance are probably roughly comparable to the FluView deaths, the larger number, the 188,000 pneumonia and influenza deaths per year. The language “roughly” is used because the April 2020 guidance appears to strongly encourage physicians and others to assign COVID-19 as the underlying cause of death in any death where COVID-19 is detected by tests or perhaps even just suspected, raising the possibility that heart attack and stroke deaths might be wrongly classified as COVID-19 deaths as well as the traditional pneumonia and influenza deaths that would be listed in the FluView data. These would presumably be misclassified as the COVID-19 deaths exhibiting the mysterious blood clots and other blood-related problems reported in some COVID-19 cases and deaths. Thus, the FluView death numbers may represent a lower bound on COVID-19 deaths rather than an exact baseline — unfortunately.
Ealy et al have raised the question whether the CDC complied with the Paperwork Reduction Act (PRA) and Information Quality Act (IQA) requirements in issuing the April and earlier March COVID-19 death certification guidelines, apparently without submitting these for public comment through the Federal Register as Ealy and co-authors claim is required by these federal laws.
Conclusion
Thus, due to the guidance on the death certificates from the CDC in April 2020, COVID-19 deaths on death certificates appear comparable to the larger FluView death numbers — or even larger numbers if heart attacks, strokes or other blood coagulation related deaths with a positive test or clinical diagnosis are being classified as COVID-19 deaths.
The CDC’s documents and web site are remarkably unclear, contradictory, and confusing for public health and scientific information presented to the general public, busy doctors and other medical professionals, or even research scientists — as previously noted by Peter Doshi and others.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
In spite of and even because of the stay-at-home, lockdown and other restrictions by health authorities in Santa Clara County, California (USA), there are many plausible routes for rapid efficient spread of the SARS-COV-2 virus presumed to cause COVID-19 in the county. Despite this, total deaths attributed to COVID-19 in the year 2020 remained remarkably low, comparable to expected deaths from pneumonia and influenza in prior years. This may of course change in the coming year.
Many probable routes of transmission are discussed and illustrated with pictures below.
Many Seeming Routes for Rapid Spread of the Disease
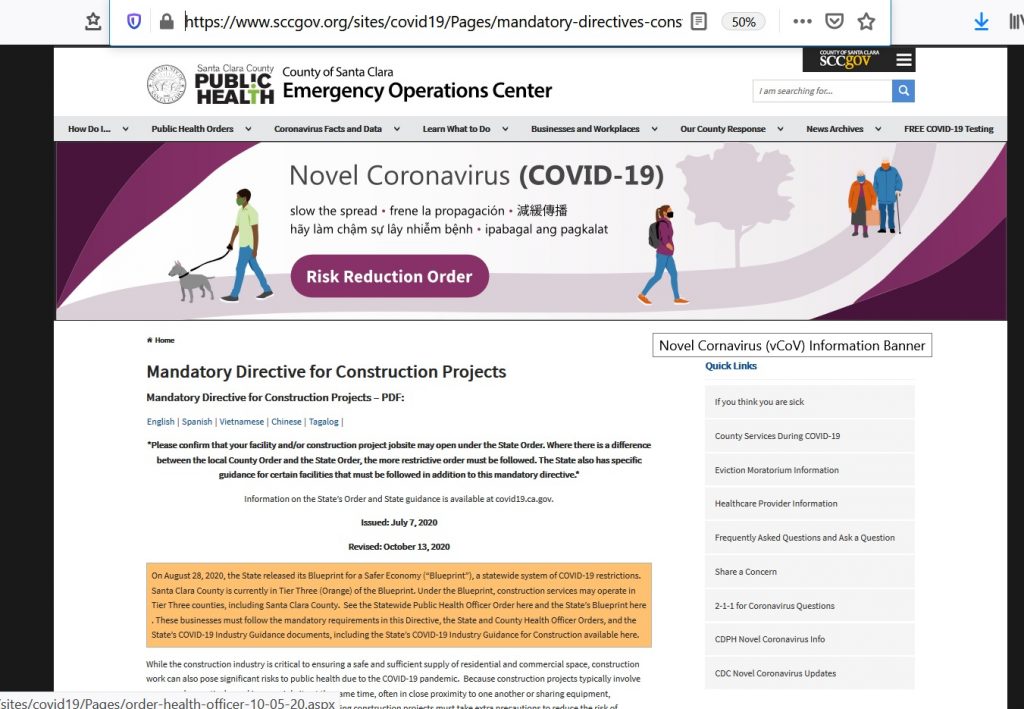
Santa Clara County, California (United States) continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May. The lockdown herds large numbers of citizens into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease. The lockdown also confines a large proportion of residents to large apartment complexes with many seemingly easy routes of transmission. “Essential” workers and others continue to use the county bus service which confines workers and others to an enclosed shared space for many minutes each day.
Ongoing Construction Projects
Santa Clara County continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May — several weeks after the original lockdown order. On a personal note, a four-story luxury apartment building construction project with at least a dozen workers every weekday from about 7:30 am to 4:30 pm has continued across the street from my apartment building since the original lockdown order except for the brief shutdown in May.
Santa Clara County Allows Construction Projects Despite COVID-19Over a Dozen Construction Workers Arriving for Work on Luxury Apartment Project in Santa Clara County, CA (August 6, 2020)Construction Workers in Close Proximity (Santa Clara County, Dec. 7, 2020)
Herding Residents into Big Box Retail Stores
The lockdown continues to herd large numbers of citizens in Santa Clara County into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease.
Safeway with Over Thirty Cars in Parking Lot (about 9:30 AM, December 7, 2020, Santa Clara County)
These giant “Big Box” retail stores have heavily used shared spaces and surfaces where one would expect the virus will rapidly spread. These include the entry/exit door areas, checkout counters, and refrigerators with popular products such as milk purchased by a large fraction of the customers and with door handlesthat all purchasers must use. These large stores often have hundreds of patrons in the store at the same time — all day, seven days per week.
Milk and other dairy products in a refrigerator with door handle that customers must use
In Santa Clara County, the lockdowns have closed or heavily curtailed restaurants, popular with the large population of single people and leading to a large increase in demand for microwave dinners often found in store refrigerators with door handles that must be used by the customers.
Microwave dinners in store refrigerator with door handle that customers must use
Several other specific scenarios exist for rapid efficient spread of the virus through these giant retail stores.
Bus Service for “Essential” Workers and Others
Santa Clara County also has a bus service, the VTA or Valley Transportation Authority, in widespread use with patrons, often “essential workers,” sharing an enclosed space and seats.
VTA Bus in Operation on December 7, 2020, Santa Clara County, California
Giant Apartment Complexes are Common in Santa Clara County
The lockdown shelter in place and stay at home orders confine “non-essential workers” to numerous generally large apartment complexes, often with hundreds of tenants, possibly thousands in some cases. In Mountain View, California — site of Google’s headquarters — about fifty-eight percent of residents (Town Charts, see Figure 5) are renters, most in large complexes. These complexes feature shared trash chutes/rooms, laundry rooms, hallways and lobbies with exterior doors and fire doors that must be opened by hand in most cases, providing many shared surfaces and spaces for spread of the virus.
Typical Trash Chute Room with Fire Door in Santa Clara County — Note Door Handle (December 7, 2020)Typical Trash Room Interior with Trash Chute (Note Handle) in Santa Clara County (December 7, 2020)Typical Laundry Room Door with Handle in Santa Clara County (December 7, 2020)
Note that fire regulations require closely spaced closed fire doors in the interior hallways — with handles or knobs that all residents must use to open the fire doors.
The large apartment complexes common in Santa Clara County provide numerous shared spaces where aerosol virus particles can collect and linger in the air as well as shared surfaces such as door handles that all residents must touch.
Gloves are not required. Gloves would have to be handled carefully and sterilized before and after each or nearly each use to avoid spreading the virus, something probably impractical and certainly currently NOT done by most residents.
In general, the apartment complex support staff cannot clean each door handle after each use. The shared support staff themselves are a high risk of both becoming infected and spreading the infection to other residents. Almost none have training or experience in bio-safety measures.
Conclusion
Despite hyperbolic headlines and reasonable expectations, deaths attributed to COVID-19 have remained remarkably low in 2020, although that may — of course — change. We will see if the usual winter surge in cases and deaths from respiratory illnesses subsides for COVID-19 or not. Prediction is notoriously difficult — especially about the future. As demonstrated above, this appears to have been in spite of rather than because of the stay-at-home and lockdown measures.
The reasons for this remarkably low death rate in Santa Clara County in 2020 remain unknown. Possible explanations include the bright sunny climate — among the most pleasant in the world, close long term past contact with China contributing to a high pre-existing immunity or resistance to SARS type coronaviruses in general, some genetic or cultural difference in Santa Clara County’s heavily Asian population (death rates in Japan and other Asian nations have been quite low compared to the United States or Europe if official figures are to be believed), better treatment of patients such as avoiding intubation, higher consumption of vitamin D by the health conscious residents, or some other cause.
(C) 2021 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
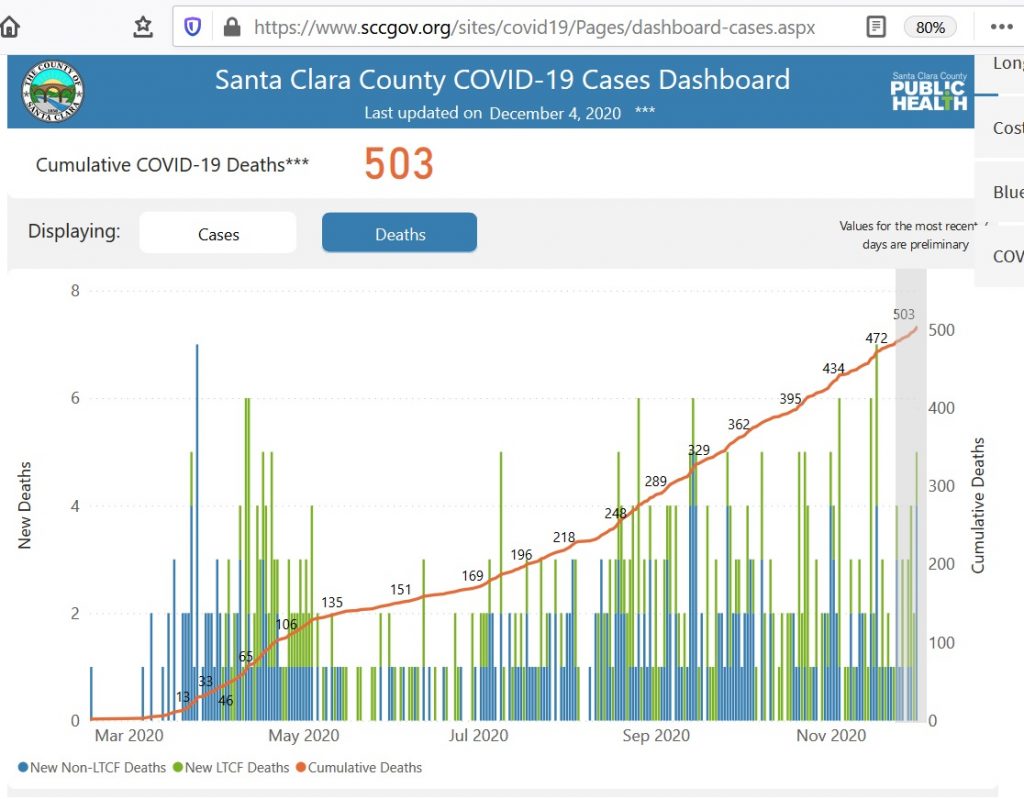
Despite frightening headlines and increased lockdown orders, total COVID-19 deaths in Santa Clara County, California remain remarkably low with total officially reported deaths of only 503 in a county with 1.9 million and close contact with China, the presumed source of the pandemic. This is a number comparable to the number of expected deaths in the county from ordinary pneumonia and influenza based on previous years.
The county continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May. The lockdown continues to herd large numbers of citizens into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease.
Subscribe to our free Weekly Newsletter for articles and videos on practical mathematics, Internet Censorship, ways to fight back against censorship, and other topics by sending an email to: subscribe [at] mathematical-software.com
Despite frightening headlines and increased lockdown orders, total COVID-19 deaths in Santa Clara County, California remain remarkably low with total officially reported deaths of only 503 in a county with 1.9 million and close contact with China, the presumed source of the pandemic. This is a number comparable to the number of expected deaths in the county from ordinary pneumonia and influenza based on previous years.
The county continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May. The lockdown continues to herd large numbers of citizens into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease.
This is the Santa Clara County COVID-19 Cases Dashboard (Deaths) on Friday, December 4, 2020.
The scary red line is the CUMULATIVE NUMBER OF COVID-19 DEATHS which is guaranteed to never decrease even if the disease disappears. It is NOT the number of daily deaths or a smoothed average of the number of daily deaths, an easy mistake when viewing graphs of this type. This means a total of 503 official COVID-19 deaths since the beginning of 2020.
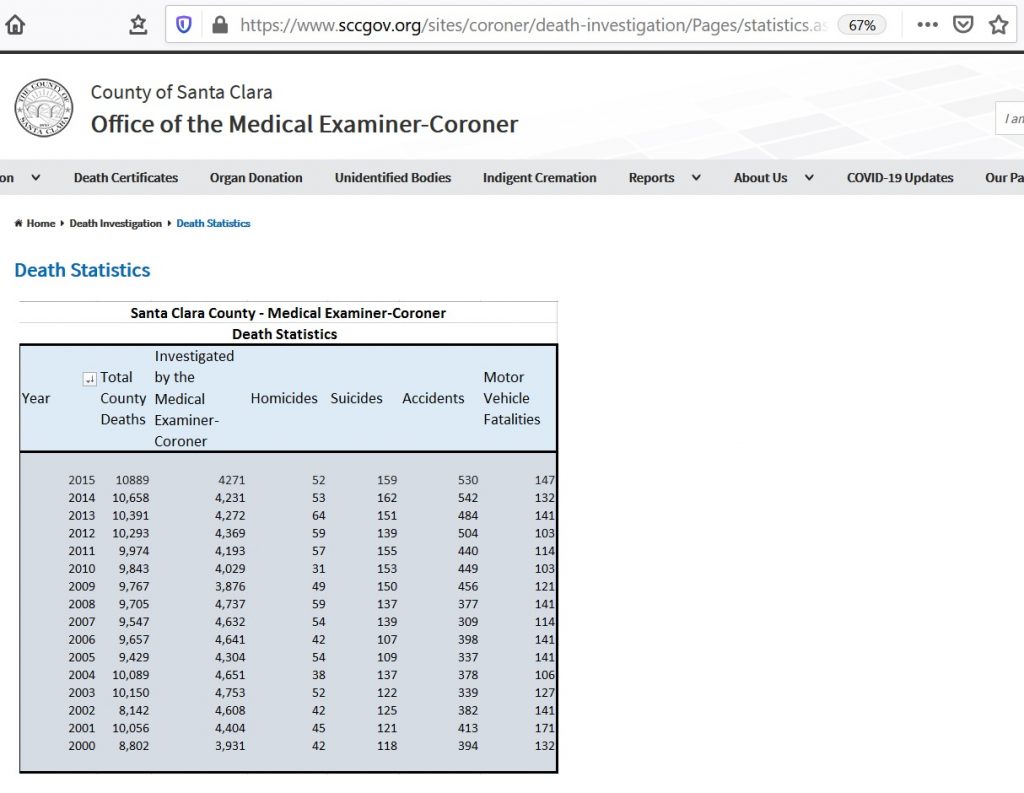
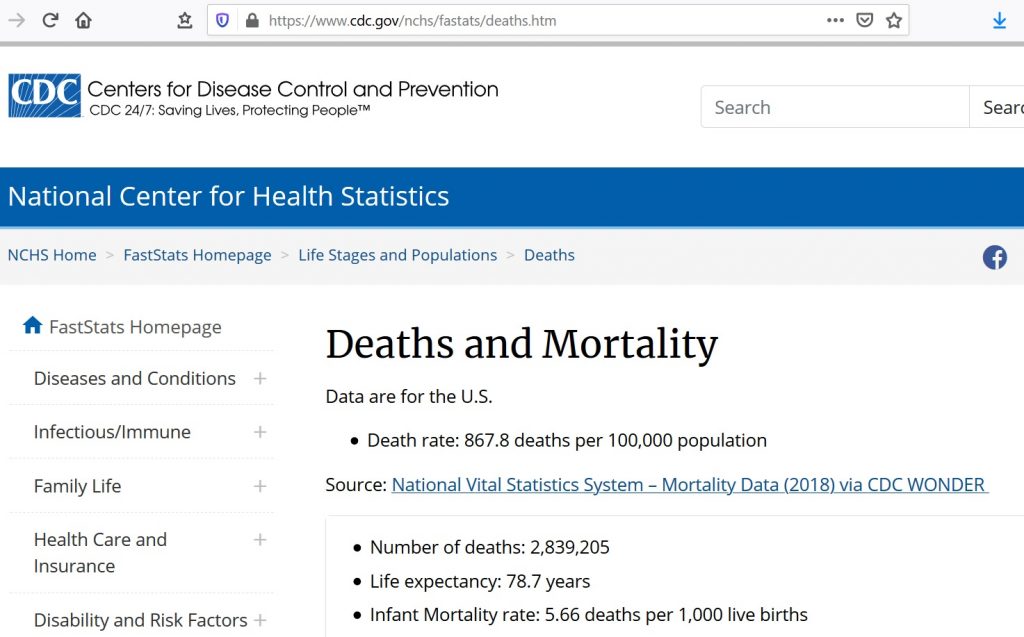
Santa Clara County has a population of about 1.9 million people in 2019 according to the US Census with 10,889 total deaths in 2015, the last year for which I could find an exact death count, according to the Office of the Medical Examiner-Coroner for the County of Santa Clara. The most recent estimated death rate for the United States in 2018 was 867.8 deaths per 100,000 people according the US Centers for Disease Control. One point nine million (1.9 million) is nineteen (19) times 100,000. This means an estimated number of deaths in Santa Clara County of nineteen (19) times 867.8 or 16,488 expected deaths in 2020 from all causes.
What percentage of these 16,488 expected deaths would be attributed to pneumonia and influenza in pre-COVID-19 years (2019 and earlier)? The CDC FluView web site shows that six to ten percent of deaths, varying seasonally, are due to pneumonia and influenza (P&I) according to the vertical axis label on the FluView Pneumonia & Influenza Mortality plot, meaning at least six percent of the deaths or 989 deaths would be due to pneumonia and influenza.
US Centers for Disease Control (CDC) FluView Pneumonia & Influenza Mortality Plot (Dec. 4, 2020)
In contrast, the CDC’s leading causes of death report Table C, Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine (see screenshot below) attributes only two percent of annual deaths (about 55,000 in 2017) to “influenza and pneumonia.” If this smaller number is used, we would expect about 329 deaths from pneumonia and influenza in 2020.
The difference between the CDC FluView and leading causes of death report numbers is probably due to the requirement that pneumonia or influenza be listed as “the underlying cause of death” in the leading causes of death report and only “a cause of death” in the FluView data. This is not clear. Many deaths have multiple “causes of death.” The assignment of an “underlying cause of death” may be quite arbitrary in some cases. Despite this, none of these official numbers either in the leading causes of death report or the FluView web site are reported with error bars or error estimates as required by common scientific and engineering practice when numbers are uncertain.
Screenshots of the official CDC, Santa Clara County, and US Census web sites used for these numbers from Friday, December 4, 2020:
Santa Clara County Total Reported Deaths from 2000 to 2015Santa Clara County Population from US Census BureauUS Centers for Disease Control (CDC) FluView Pneumonia and Influenza Mortality Plots (Dec. 4, 2020)United States National Death Rate According to US CDC (Dec. 4, 2020)US CDC Leading Causes of Death Report Attributes Only About Two Percent of All Deaths to Pneumonia and Influenza (Line Item 8: Influenza and Pneumonia) — not the Six to Ten Percent in the FluView Graphs
Remarkably the total number of deaths (503) attributed to COVID-19 in Santa Clara County is clearly within the range of deaths expected from pneumonia and influenza (329 to 989) based on historical data prior to 2020.
Santa Clara County Has Close Ties to China
Santa Clara County, home to Apple, Google, and many other companies with extensive manufacturing operations in China, the presumed source of the Sars-COV-2 virus, and large numbers of direct and contract employees again from China (mainland China), has extensive ties to China, meaning mainland China, not just Taiwan, Singapore, Hong Kong, and other ethnically Chinese nations and communities outside of China proper. Indeed, it probably has the closest ties, travel and trade to and from China of any region in the United States — likely much more than the New York and New Jersey region where the most deaths and highest death rates have been reported. One would expect Santa Clara County, California to have the earliest and largest cumulative number of deaths from COVID-19 in the United States.
According to the New York Times (April 4, 2020), at least 430,000 people returned to the United States from China after the Sars-COV-2 virus appeared, many after President Trump’s travel ban. A large fraction of these probably returned to Santa Clara County given the close ties between China and Santa Clara County. According to the San Francisco Chronicle, the first US COVID case was a 57-year old woman who passed away at home on February 6, 2020, well before the Kirkland Life Care Center cases in late February.
Many Seeming Routes for Rapid Spread of the Disease
Santa Clara County continues to authorize many luxury apartment and other construction projects with teams of workers in close proximity five full days per week, after a brief 3-4 week shutdown in May — several weeks after the original lockdown order. On a personal note, a four-story luxury apartment building construction project with at least a dozen workers every weekday from about 7:30 am to 4:30 pm has continued across the street from my apartment building since the original lockdown order except for the brief shutdown in May.
Santa Clara County Allows Construction Projects Despite COVID-19Over a Dozen Construction Workers Arriving for Work on Luxury Apartment Project in Santa Clara County, CA (August 6, 2020)Construction Workers in Close Proximity (Santa Clara County, Dec. 7, 2020)
The lockdown continues to herd large numbers of citizens in Santa Clara County into a few gigantic stores such as Safeway, Walmart, and Target, enabling what would seem like an efficient route for rapid spread of the disease.
Safeway with Over Thirty Cars in Parking Lot (about 9:30 AM, December 7, 2020, Santa Clara County)
UPDATE (Dec. 9, 2020): These giant “Big Box” retail stores have heavily used shared spaces and surfaces where one would expect the virus will rapidly spread. These include the entry/exit door areas, checkout counters, and refrigerators with popular products such as milk purchased by a large fraction of the customers and with door handlesthat all purchasers must use. These large stores often have hundreds of patrons in the store at the same time — all day, seven days per week.
Milk and other dairy products in a refrigerator with door handle that customers must use
In Santa Clara County, the lockdowns have closed or heavily curtailed restaurants, popular with the large population of single people and leading to a large increase in demand for microwave dinners often found in store refrigerators with door handles that must be used by the customers.
Microwave dinners in store refrigerator with door handle that customers must use
Several other specific scenarios exist for rapid efficient spread of the virus through these giant retail stores.
UPDATE (Dec. 6, 2020): Santa Clara County also has a bus service, the VTA or Valley Transportation Authority, in widespread use with patrons, often “essential workers,” sharing an enclosed space and seats.
VTA Bus in Operation on December 7, 2020, Santa Clara County, California
UPDATE (Dec. 7, 2020) The lockdown shelter in place and stay at home orders confine “non-essential workers” to numerous generally large apartment complexes, often with hundreds of tenants, possibly thousands in some cases. In Mountain View, California — site of Google’s headquarters — about fifty-eight percent of residents (Town Charts, see Figure 5) are renters, most in large complexes. These complexes feature shared trash chutes/rooms, laundry rooms, hallways and lobbies with exterior doors and fire doors that must be opened by hand in most cases, providing many shared surfaces and spaces for spread of the virus.
Typical Trash Chute Room with Fire Door in Santa Clara County — Note Door Handle (December 7, 2020)Typical Trash Room Interior with Trash Chute (Note Handle) in Santa Clara County (December 7, 2020)Typical Laundry Room Door with Handle in Santa Clara County (December 7, 2020)
Note that fire regulations require closely spaced closed fire doors in the interior hallways — with handles or knobs that all residents must use to open the fire doors.
The large apartment complexes common in Santa Clara County provide numerous shared spaces where aerosol virus particles can collect and linger in the air as well as shared surfaces such as door handles that all residents must touch.
Gloves are not required. Gloves would have to be handled carefully and sterilized before and after each or nearly each use to avoid spreading the virus, something probably impractical and certainly currently NOT done by most residents.
In general, the apartment complex support staff cannot clean each door handle after each use. The shared support staff themselves are a high risk of both becoming infected and spreading the infection to other residents. Almost none have training or experience in bio-safety measures.
These shared spaces and surfaces are enclosed, protected from exterior wind that can disperse the virus particles and from the ultraviolet component of sunlight which can destroy the virus particles outside. By design, the required fire doors limit air flow in the buildings to prevent a disastrous fire. Citizens are being mandated/encouraged to spend most of their time inside in these complexes.
Conclusion
As of December 4, 2020, the total and daily death numbers for COVID-19 continue to deviate sharply from both hyperbolic headlines and reasonable expectations — as was the case in March and April of 2020. Indeed, the total number of official reported COVID-19 deaths to date (503 on Dec. 4, 2020) remains small enough to be consistent with no new or unusual disease causing more deaths than normal in Santa Clara County in 2020.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
How Reliable are the US Centers for Disease Control’s Death Numbers
A short video showing the contradictory pneumonia and influenza death numbers on the CDC web site and official documents. The FluView web site claims six to ten percent of all deaths are due to pneumonia and influenza in a prominently displayed graphic. However, the Leading Causes of Death report claims about two percent of deaths are caused by pneumonia and influenza, less than one third of the percentages reported on the FluView web site. Detailed references are provided below.
Looking at the numbers behind the percentages. The CDC uses two grossly contradictory numbers of annual deaths from pneumonia and influenza: about 55,000 in the annual leading causes of the death report and about 188,000 in National Center for Health Statistics (NCHS) data used on the FluView web site to report the percentage of deaths each week due to pneumonia and influenza. These differ by a factor of OVER THREE. The larger FluView number is comparable to the current cumulative total COVID-19 deaths in the United States.
The most recent raw data appears to still be accessible on the FluView Pneumonia and Influenza Mortality web page:
See Table C: Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 (Page 9 of PDF)
Line item 8 “Influenza and pneumonia” lists 55,672 deaths in 2017
Leading Causes of Death Table C for 2017 (Note the line item “Influenza and pneumonia” with only 2.0 percent of deaths due to pneumonia and influenza)
The most likely reason for the gross discrepancy between the FluView percentages and death numbers and the leading causes of death is that the FluView graphic counts any death certificate with pneumonia or influenza listed as “a cause of death.” Death certificates often list multiple causes of death. The leading causes of death report appears to list only death certificates that list pneumonia or influenza as the “underlying cause of death,” which may be a rather arbitrary assignment of causation to a single cause of death. While the fine print seems to say this, it is ambiguous.
Consequentially, the CDC death numbers can vary enormously depending on the definition of cause of death — or some other reason that is not clearly documented in the CDC documents. This is discussed further in the associated video.
A significant question is what fraction of the numbers, especially on the FluView web site, are due to opportunistic infections where the immune system or general health is so weakened by some other cause such as chemotherapy, AIDS, cancer, the aging process etc. that death is likely or inevitable and multiple infections may be present. The likely purpose of the FluView graphic and numbers is to frighten the public into purchasing the flu vaccine — which is unlikely to work for patients whose immune system weakens or fails.
Peter Doshi’s Critiques of US Flu Death Numbers
Are US flu death figures more PR than science? British Medical Journal (2005)
Impact of Influenza Vaccination on Seasonal Mortality in the US Elderly Population Lone Simonsen, PhD; Thomas A. Reichert, MD, PhD; Cecile Viboud, PhD; et al William C. Blackwelder, PhD; Robert J. Taylor, PhD; Mark A. Miller, MD Arch Intern Med. 2005;165(3):265-272. doi:10.1001/archinte.165.3.265
Subscribers gain access to the advanced professional features of our censored search web site and service — https://censored-search.com — a search engine for censored Internet content banned or shadow-banned by increasingly censored, advertising beholden social media and search engines such as Google, YouTube, and Facebook. The free version of censored-search.com — available to all — uses a modified page rank algorithm, essentially a popularity contest. The paid professional version includes advanced search algorithms to find and prioritize content that is probably being censored by vested interests because it is useful and true — for example, evidence that a product or service is harmful to users.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The CDC’s Grossly Contradictory Death Numbers (Click on Image to View the Video)
The CDC uses two grossly contradictory numbers of annual deaths from pneumonia and influenza: about 55,000 in the annual leading causes of the death report and about 188,000 in National Center for Health Statistics (NCHS) data used on the FluView web site to report the percentage of deaths each week due to pneumonia and influenza. These differ by a factor of OVER THREE. The larger FluView number is comparable to the current cumulative total COVID-19 deaths in the United States (Aug 30, 2020).
Since it is generally agreed that lockdowns and quarantines are not justified for a disease similar to typical annual pneumonia and influenza deaths, the reasons for this gross contradiction in the two annual death numbers should be resolved. Is it correct to compare the COVID-19 death numbers to the FluView number, the leading causes of death number, or some other number and, if so, exactly why and how?
Video Transcript: The CDC uses two grossly contradictory numbers of annual deaths from pneumonia and influenza: about 55,000 in the annual leading causes of the death report and about 188,000 in National Center for Health Statistics (NCHS) data used on the FluView web site to report the percentage of deaths each week due to pneumonia and influenza. These differ by a factor of OVER THREE.
This is the leading causes of death report for 2017 on the CDC web site. Table C: Deaths and percentage of total deaths for the 10 leading causes of death: United States, 2016 and 2017 on Page Nine. Note line item number 8 “pneumonia and influenza” with 55,672 deaths in 2017. Also note 2,813,503 deaths from all causes in 2017.
This is the CDC FluView web site. The red line purports to be the percentage of weekly deaths caused by pneumonia and influenza. It varies seasonally and averages about six percent over a year. Six percent of the 2,813,503 deaths in 2017 is 168,810 deaths, over three times the 55,672 deaths in the leading causes of death report.
The actual numbers are available here in data files from the National Center for Health Statistics (NCHS). These give about 188,000 deaths from pneumonia and influenza in 2017. The death numbers for other years are quite similar.
To be clear, the leading causes of deaths report gives 55,672 deaths from pneumonia and influenza in 2017.
The average six percent of deaths from the FluView Graph means about 170,000 deaths must have been due to pneumonia and influenza — NOT 55,000. In fact, the raw data from the NCHS on the sites gives just about 188,000 deaths due to pneumonia and influenza in 2017, over THREE TIMES the number of deaths in the leading causes of death report and the widely quoted estimated deaths from flu from the CDC.
This means the number of pneumonia and influenza deaths must be highly arbitrary, dependent on unstated definitions, or there are gross counting errors. The larger FluView number of 188,000 is comparable to the current total of COVID-19 deaths in the US which is often compared to a smaller number of flu deaths each year similar to the leading causes of deaths number of 55,000.
Since it is generally agreed that lockdowns and quarantines are not justified for a disease similar to typical annual pneumonia and influenza deaths, the reasons for this gross contradiction in the two annual death numbers should be resolved. Is it correct to compare the COVID-19 death numbers to the FluView number, the leading causes of death number, or some other number and, if so, exactly why and how?
The most recent raw data appears to still be accessible on the FluView Pneumonia and Influenza Mortality web page:
Subscribers gain access to the advanced professional features of our censored search web site and service — censored-search.com — a search engine for censored Internet content banned or shadow-banned by increasingly censored, advertising beholden social media and search engines such as Google, YouTube, and Facebook. The free version of censored-search.com — available to all — uses a modified page rank algorithm, essentially a popularity contest. The paid professional version includes advanced search algorithms to find and prioritize content that is probably being censored by vested interests because it is useful and true — for example, evidence that a product or service is harmful to users.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).