
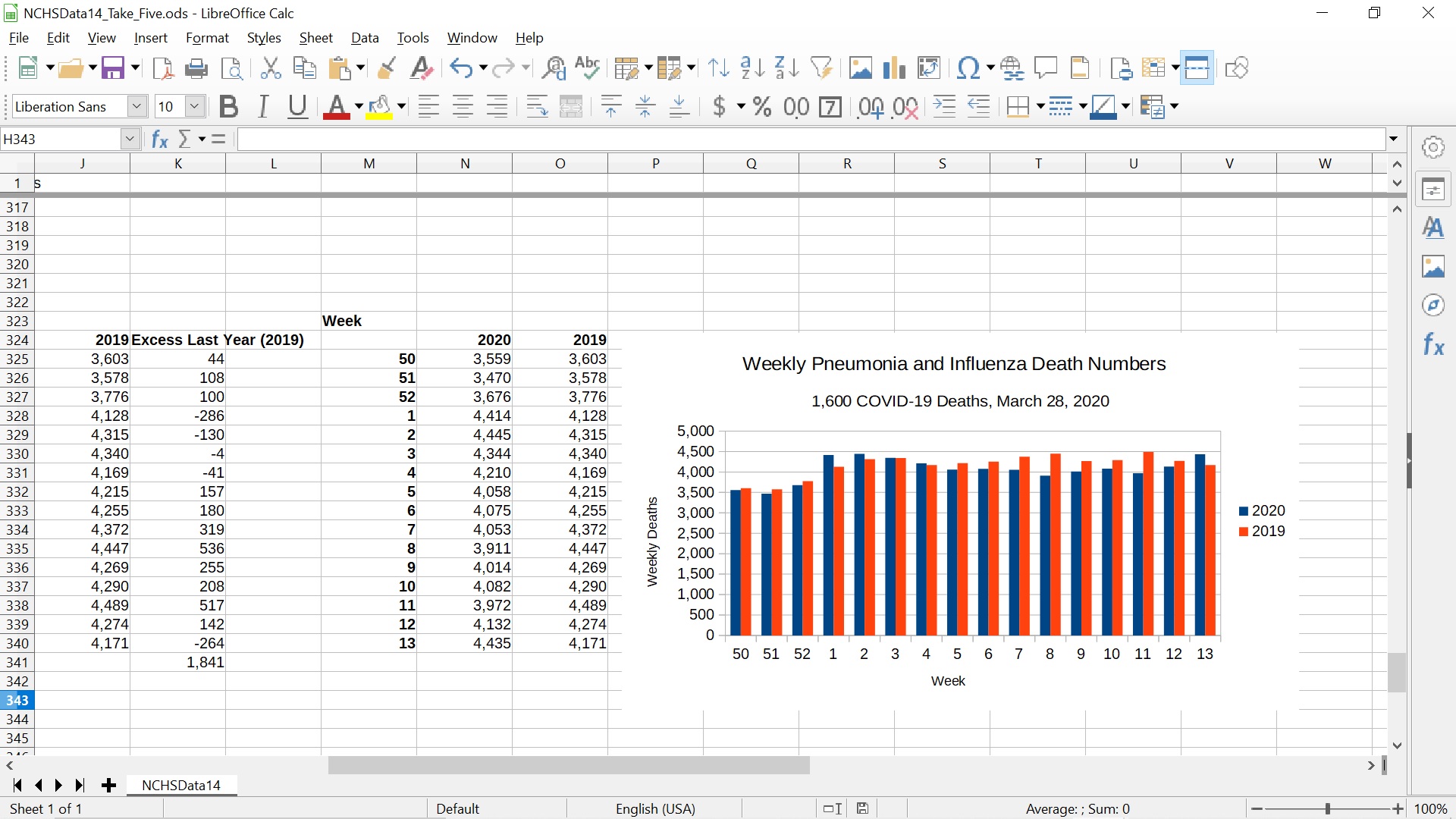

The updated plot is from a LibreOffice spreadsheet which can be downloaded at the link below. LibreOffice is a free, open-source alternative to Microsoft Office. It is available for Microsoft Windows, Mac OS X, and most flavors of Unix. It can be downloaded here.
The original data is from https://www.cdc.gov/flu/weekly/weeklyarchives2019-2020/data/NCHSData14.csv
The companion video for this article is at: https://youtu.be/DcjeKzmLjz8 and https://www.bitchute.com/video/LvKUWJOxcTSq/ The video is about sixteen minutes long. It is usually faster to read the written article than listen to the companion video.
I made a mistake copying the column of pneumonia and influenza deaths from early 2019 (weeks 1-13 of 2019 and weeks 50-52 of 2020) with LibreOffice Calc (the spreadsheet). The spreadsheet copied the macros in the cells instead of the number values. These macros were then applied to the columns to the left of the copied column, giving incorrect values that exaggerated the excess of deaths in comparable weeks last year (2019).
The actual excess is 1,841 more deaths in 2019, not about 6,000.
I was using the spreadsheet to make the results more accessible to a general audience. The copying error was consistent with the results from the more in-depth Python data analysis. In retrospect I should have checked the spreadsheet numbers more carefully.
Discussion
This does not change the conclusion that there is no sign of COVID-19 in the numbers until March 14, 2020 and a weak rise consistent with normal fluctuations in the weekly numbers in the final two weeks (March 14-28, 2020, weeks 12 and 13). It does reduce the size of the discrepancy between the two years. It remains possible that all the about 1,600 COVID-19 deaths reported as of March 28, 2020 could be conventional pneumonia and influenza deaths labeled as COVID-19 due to false positive RT-PCR tests and other misdiagnoses.
As I have discussed, there are strong reasons to doubt the CDC numbers. The most egregious I have found so far is the remarkable difference between the about 55,000 deaths from “influenza and pneumonia” in the leading causes of death tables (Table B, Page Six) and the about 188,000 deaths from “pneumonia and influenza” in the NCHSData14.csv file and other NCHSData<Week Number>.csv files.
An educated guess is that the 55,000 deaths from “influenza and pneumonia” is the output of a model the CDC uses to estimate the number of deaths directly or indirectly caused by “influenza viruses.” In the weekly pneumonia and influenza death numbers, the vast majority of deaths are listed as pneumonia and not the separate “influenza” category. Thus about 130,000 deaths appear to have been assigned to other categories in the final deaths for 2017 report, possibly “chronic lower respiratory diseases” which is the fourth (4th) leading cause of death. This is however a theory and CDC should carefully clarify what they are doing.
Accordingly, it is difficult to know what pre-processing or modeling/estimation may have been applied to the weekly pneumonia and influenza death numbers, although the commentary on the CDC web site implies these numbers are counts of death certificates and the causes of death on death certificates reported to the CDC by state and local authorities.
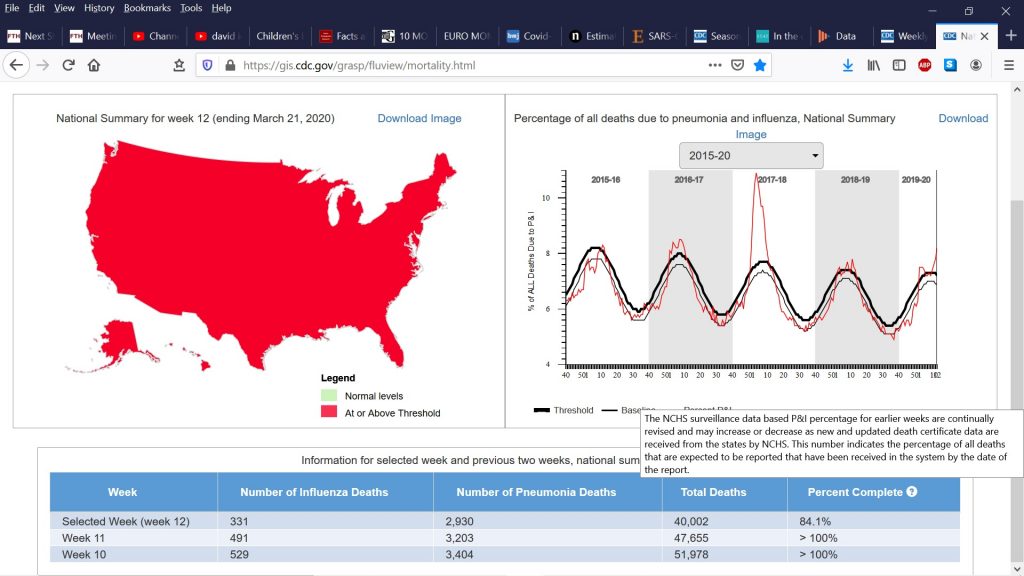
I am looking through the NCHSData<Week Number>.csv files to see how complete they may actually be. The FluView web page contains a table that seems to imply that all weeks except the very last week in the file are complete or almost complete. They use the label “> 100%” where > is presumably “greater than”. Of course, 100 percent usually means complete.
There are many possible reasons for COVID-19 deaths not showing up in the weekly pneumonia and influenza death numbers before March 14, 2020 despite the Chinese coverup in December and early January, the US testing fiasco, the 430,000 visitors to the United States from China since the coronavirus surfaced, and the many asymptomatic carriers now being detected. These different possible reasons have different, even opposite in some cases, implications for public health policy.
Possible reasons include:
Despite the many problems above, the public health authorities have been remarkably successful in identifying nearly all COVID-19 deaths up to March 14, 2020. This seems too good to be true, but cannot be excluded.
The infection fatality rate (aka actual mortality rate) of the COVID-19 coronavirus is much less than early numbers such as 3.4 percent from the World Health Organization (WHO) or the 0.9-1 percent used by various authorities. Iceland, South Korean, Denmark and German data suggest about 0.5 percent mortality rate – which still could be higher than real rate.
Many COVID-19 deaths are due to aggressive treatment of the disease, e.g. intubation, rather than the disease alone.
The weekly pneumonia and influenza death numbers are substantially incomplete, due to normal delays or due to unusual delays associated with the crisis.
There has been a compensating drop in non-COVID pneumonia and influenza deaths due to shelter-in-place and taking it easy. Elderly and susceptible persons may have taken precautions in January and February due to the publicity, even before the shutdown in mid March.
Something else
Some combination of some or all of the above!
Conclusion
There is a remarkable lack of key measurements in the current coronavirus COVID-19 pandemic. These include the actual mortality rate (aka infection fatality rate) broken down by age, sex, race, pre-existing medical conditions, ambient temperature, sunlight levels, pollution levels, and other risk factors. The false positive and false negative rates of the tests for the disease, both the tests for an active infection such as the RT-PCR tests and tests for past infection such as the antibody tests. The methods and rates of transmission for the disease. Aerosol transmission probably occurs at least at a low level and is virtually unstoppable.
It is important to collect this data and measure these key parameters as quickly as possible in an open, “transparent” manner with multiple independent teams, not all funded or controlled by the CDC, as soon as possible to make good decisions based on knowledge and data, rather than fear, ignorance, and the primal fight or flight response.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).