A key question about the coronavirus COVID-19 pandemic and pneumonia and influenza deaths in general is the role of air pollution in the disease and deaths. Wuhan, China — the presumed source of the outbreak — had high levels of pollution resulting in mass protests in July of 2019 and the hard hit Lombardy region of Italy had some of the highest air pollution levels in Europe. There are many kinds of air pollution and how they interact with the lungs, immune system, and various infections is unclear. There is a long body of research that air pollution increases the risk and severity of pneumonia.
I have listed several popular and scientific articles on air pollution and the coronavirus or pneumonia in general below. I also included several articles from 2019 on the protests in Wuhan at the end.
Keep in mind when medical scientists and the press say “linked” or “associated” this usually mean a statistical correlation has been found. Correlation (even perfect correlation) does not prove causation.
This New York Times article is about the Harvard research listed below in the Scientific Articles section.
Conclusions: A small increase in long-term exposure to PM2.5 leads to a large increase in COVID-19 death rate, with the magnitude of increase 20 times that observed for PM2.5 and all-cause mortality. The study results underscore the importance of continuing to enforce existing air pollution regulations to protect human health both during and after the COVID-19 crisis. The data and code are publicly available.
“Does air pollution make you more susceptible to coronavirus? California won’t like the answer” by Tony Barboza, March 21, 2020, LA Times
A relatively recent study at McMaster University in Canada linking air pollution to pneumonia.
Scientific Articles
Exposure to air pollution and COVID-19 mortality in the United States (Updated April 5, 2020)
Xiao Wu MS, Rachel C. Nethery PhD, M. Benjamin Sabath MA, Danielle Braun PhD, Francesca Dominici PhD All authors are part of the Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, MA, 02115, USA
Lead authors: Xiao Wu and Rachel C. Nethery Corresponding and senior author: Francesca Dominici, PhD
Conclusions: A small increase in long-term exposure to PM2.5 leads to a large increase in COVID-19 death rate, with the magnitude of increase 20 times that observed for PM2.5 and all-cause mortality. The study results underscore the importance of continuing to enforce existing air pollution regulations to protect human health both during and after the COVID-19 crisis. The data and code are publicly available.
Conclusions: Increased rates of culture-negative pneumonia and influenza were associated with increased PM2.5 concentrations during the previous week, which persisted despite reductions in PM2.5 from air quality policies and economic changes. Though unexplained, this temporal variation may reflect altered toxicity of different PM2.5 mixtures or increased pathogen virulence.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
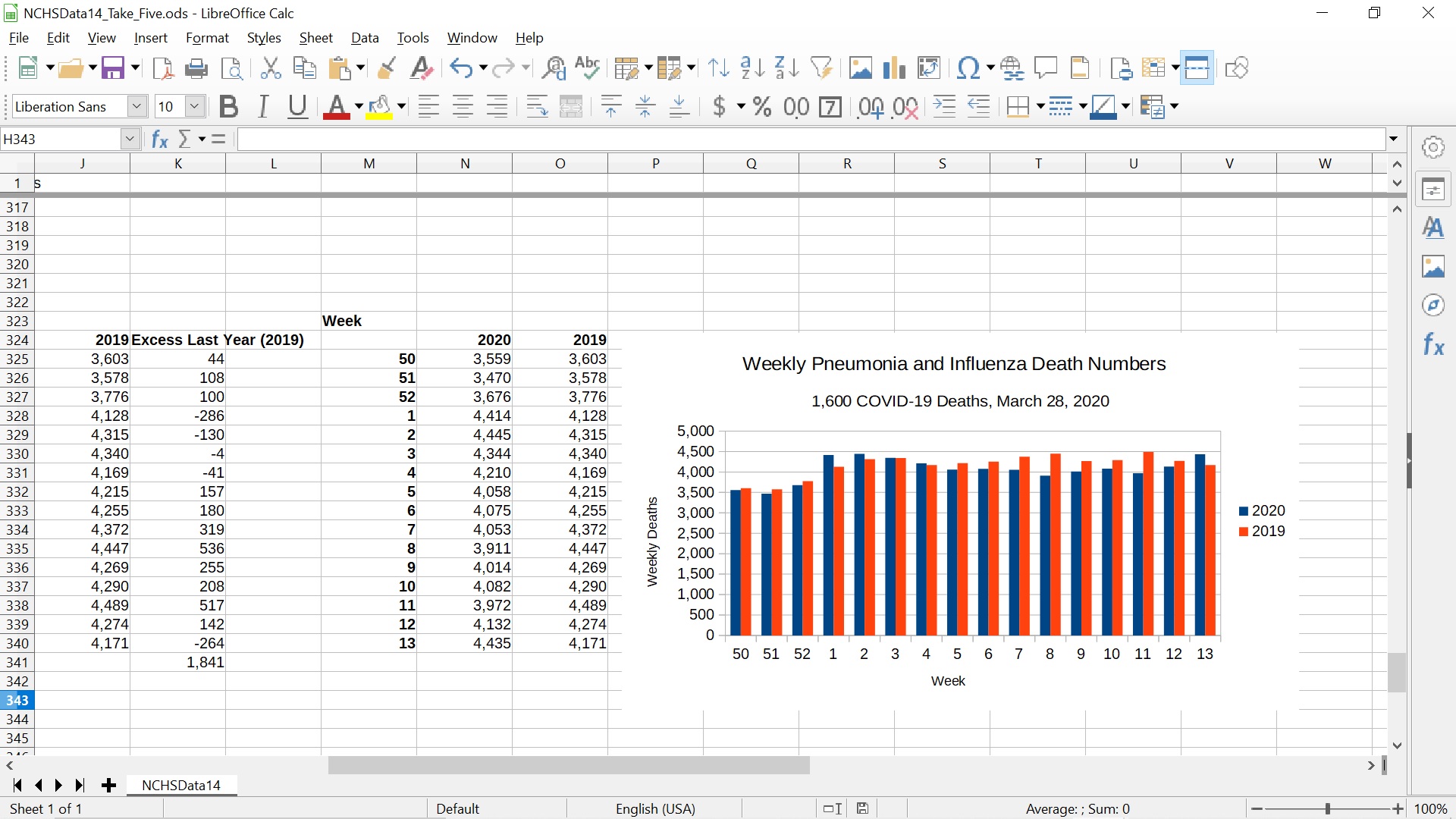
Weekly Pneumonia and Influenza Death Numbers for 2020 and 2019 Compared
The updated plot is from a LibreOffice spreadsheet which can be downloaded at the link below. LibreOffice is a free, open-source alternative to Microsoft Office. It is available for Microsoft Windows, Mac OS X, and most flavors of Unix. It can be downloaded here.
I made a mistake copying the column of pneumonia and influenza deaths from early 2019 (weeks 1-13 of 2019 and weeks 50-52 of 2020) with LibreOffice Calc (the spreadsheet). The spreadsheet copied the macros in the cells instead of the number values. These macros were then applied to the columns to the left of the copied column, giving incorrect values that exaggerated the excess of deaths in comparable weeks last year (2019).
The actual excess is 1,841 more deaths in 2019, not about 6,000.
I was using the spreadsheet to make the results more accessible to a general audience. The copying error was consistent with the results from the more in-depth Python data analysis. In retrospect I should have checked the spreadsheet numbers more carefully.
Discussion
This does not change the conclusion that there is no sign of COVID-19 in the numbers until March 14, 2020 and a weak rise consistent with normal fluctuations in the weekly numbers in the final two weeks (March 14-28, 2020, weeks 12 and 13). It does reduce the size of the discrepancy between the two years. It remains possible that all the about 1,600 COVID-19 deaths reported as of March 28, 2020 could be conventional pneumonia and influenza deaths labeled as COVID-19 due to false positive RT-PCR tests and other misdiagnoses.
As I have discussed, there are strong reasons to doubt the CDC numbers. The most egregious I have found so far is the remarkable difference between the about 55,000 deaths from “influenza and pneumonia” in the leading causes of death tables (Table B, Page Six) and the about 188,000 deaths from “pneumonia and influenza” in the NCHSData14.csv file and other NCHSData<Week Number>.csv files.
An educated guess is that the 55,000 deaths from “influenza and pneumonia” is the output of a model the CDC uses to estimate the number of deaths directly or indirectly caused by “influenza viruses.” In the weekly pneumonia and influenza death numbers, the vast majority of deaths are listed as pneumonia and not the separate “influenza” category. Thus about 130,000 deaths appear to have been assigned to other categories in the final deaths for 2017 report, possibly “chronic lower respiratory diseases” which is the fourth (4th) leading cause of death. This is however a theory and CDC should carefully clarify what they are doing.
Accordingly, it is difficult to know what pre-processing or modeling/estimation may have been applied to the weekly pneumonia and influenza death numbers, although the commentary on the CDC web site implies these numbers are counts of death certificates and the causes of death on death certificates reported to the CDC by state and local authorities.
I am looking through the NCHSData<Week Number>.csv files to see how complete they may actually be. The FluView web page contains a table that seems to imply that all weeks except the very last week in the file are complete or almost complete. They use the label “> 100%” where > is presumably “greater than”. Of course, 100 percent usually means complete.
CDC “Percent Complete” Table (Misleading language at best)
There are many possible reasons for COVID-19 deaths not showing up in the weekly pneumonia and influenza death numbers before March 14, 2020 despite the Chinese coverup in December and early January, the US testing fiasco, the 430,000 visitors to the United States from China since the coronavirus surfaced, and the many asymptomatic carriers now being detected. These different possible reasons have different, even opposite in some cases, implications for public health policy.
Possible reasons include:
Despite the many problems above, the public health authorities have been remarkably successful in identifying nearly all COVID-19 deaths up to March 14, 2020. This seems too good to be true, but cannot be excluded.
The infection fatality rate (aka actual mortality rate) of the COVID-19 coronavirus is much less than early numbers such as 3.4 percent from the World Health Organization (WHO) or the 0.9-1 percent used by various authorities. Iceland, South Korean, Denmark and German data suggest about 0.5 percent mortality rate – which still could be higher than real rate.
Many COVID-19 deaths are due to aggressive treatment of the disease, e.g. intubation, rather than the disease alone.
The weekly pneumonia and influenza death numbers are substantially incomplete, due to normal delays or due to unusual delays associated with the crisis.
There has been a compensating drop in non-COVID pneumonia and influenza deaths due to shelter-in-place and taking it easy. Elderly and susceptible persons may have taken precautions in January and February due to the publicity, even before the shutdown in mid March.
Something else
Some combination of some or all of the above!
Conclusion
There is a remarkable lack of key measurements in the current coronavirus COVID-19 pandemic. These include the actual mortality rate (aka infection fatality rate) broken down by age, sex, race, pre-existing medical conditions, ambient temperature, sunlight levels, pollution levels, and other risk factors. The false positive and false negative rates of the tests for the disease, both the tests for an active infection such as the RT-PCR tests and tests for past infection such as the antibody tests. The methods and rates of transmission for the disease. Aerosol transmission probably occurs at least at a low level and is virtually unstoppable.
It is important to collect this data and measure these key parameters as quickly as possible in an open, “transparent” manner with multiple independent teams, not all funded or controlled by the CDC, as soon as possible to make good decisions based on knowledge and data, rather than fear, ignorance, and the primal fight or flight response.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
In coverage of the coronavirus COVID-19 pandemic, one often sees a value for the infection fatality rate (also known as the actual mortality rate, which is different from the “case fatality rate”) of 0.1 percent, meaning one in 1000 people infected by the “flu” dies. Infected includes people who are asymptomatic, have mild cases — anyone who is actually infected even if never detected. It is often explicitly or implicitly argued that if the infection fatality rate of COVID-19 is only 0.1 percent as suggested by a recent study by Stanford researchers (https://www.medrxiv.org/content/10.1101/2020.04.14.20062463v1.full.pdf) we can relax and go back to work. Unfortunately, it is probably not that simple.
We can use our prevalence estimates to approximate the infection fatality rate from COVID-19 in Santa Clara County. As of April 10, 2020, 50 people have died of COVID-19 in the County, with an average increase of 6% daily in the number of deaths. If our estimates of48,000-81,000 infections represent the cumulative total on April 1, and we project deaths to April 22 (a 3 week lag from time of infection to death22), we estimate about 100 deaths in the county. A hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%. If antibodies take longer than 3 days to appear, if the average duration from case identification to death is less than 3 weeks, or if the epidemic wave has peaked and growth in deaths is less than 6% daily, then the infection fatality rate would be lower. These straightforward estimations of infection fatality rate fail to account for age structure and changing treatment approaches to COVID-19. Nevertheless,our prevalence estimates can be used to update existing fatality rates given the large upwards revision of under-ascertainment
COVID-19 Antibody Seroprevalence in Santa Clara County, California by Bendavid et al
It is thought the vast majority of adults get at least two symptomatic “colds” or “flus” in common usage (The CDC claims adults get 2-3 “common colds” per year and children more on their web site which matches common experience.). These are caused by a wide variety of viruses and bacteria and sometimes chemical toxins. These include the rhinovirus, various coronaviruses other that the “novel” SARS-COV-2 coronavirus, and many others including a category of viruses known as “influenza” or “influenza viruses”.
With a total US population of about 330 million, we can estimate at least 660 million individual cases and separate infections of these “cold” or “flu” organisms (either viruses or bacteria) each year. This gives a naive effective infection fatality rate averaged over the population and different diseases of:
188,000 divided by 660 million is: 0.028 percent (0.00028484848484848485)
55,000 divided by 660 million is: 0.008 percent (0.00008333333333)
This is of course much less than 0.1 percent (one in 1000).
What gives?
In common English usage, the terms “cold” and “flu” are often used interchangeably. The use of the terms “flu” and “influenza” to describe respiratory illnesses that vary in incidence seasonally predates the discovery of the influenza viruses, a category of viruses that can cause these symptoms. Influenza is Italian, from the Latin “influentia,” for “influence,” referring to the baleful influence of the stars that the ancients blamed for the disease.
The CDC hopelessly blurs the distinctions, if any, between “common cold”, “cold”, “flu”, “influenza”, “influenza like illness,” “influenza associated,” “pneumonia,” and other terms in its promotional and “scientific” materials.
Influenza as in the influenza viruses is rarely listed as a cause of death on death certificates. The weekly “pneumonia and influenza” death numbers from the National Center for Health Statistics (NCHS) only list about 8,000 deaths from influenza in 2017. The CDC cites several different reasons for claiming there is massive underdiagnosis and underreporting of influenza (THE VIRUS) deaths, dating back to at least 2005 and persisting despite the CDC’s extensive educational efforts.
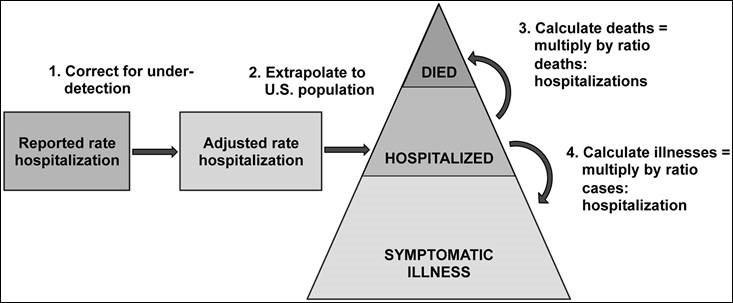
The CDC uses a mysterious model to estimate about 55,000 annual deaths from influenza (THE VIRUS). Presumably the number of deaths from “influenza and pneumonia” in the leading causes of death is this number or something closely related — but this is not clear. Incidentally, in this age of the Internet and pervasive computing, the CDC could publish the actual source code for their model in a free open-source language such as Python on their web site for all to see and review.
CDC Graphic About Influenza Model (There is a HUGE correction for under-detection)
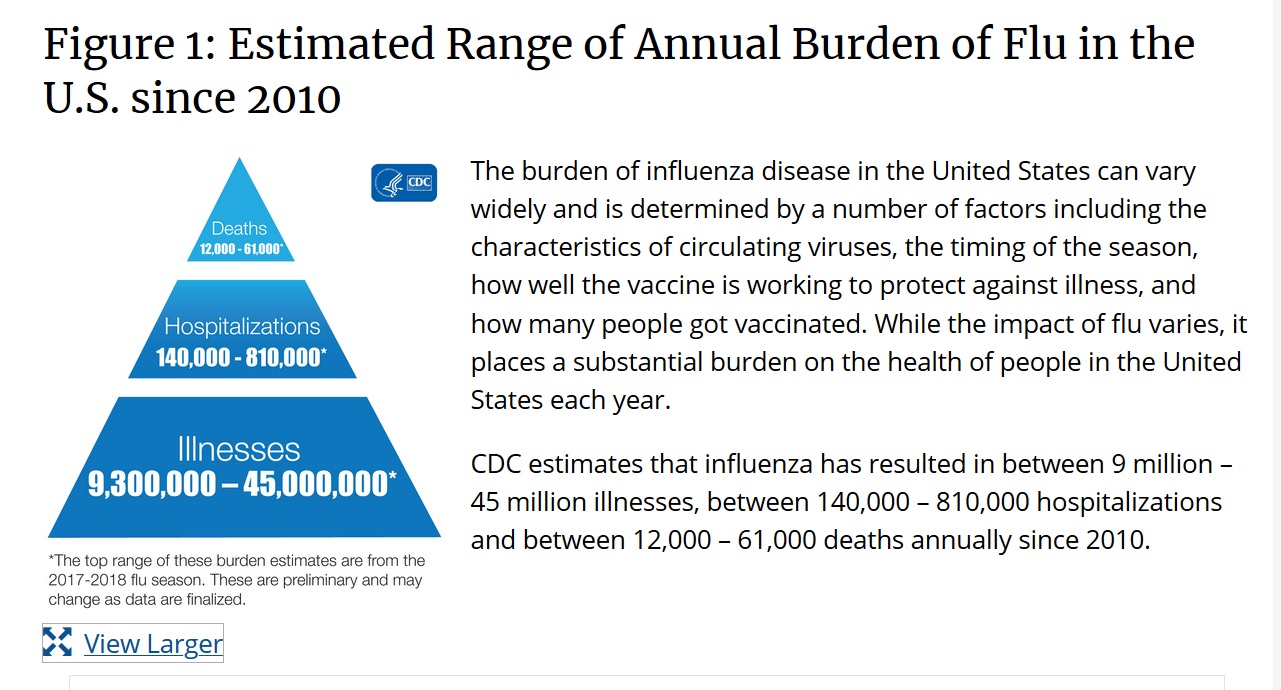
Part of this model is an estimate of how many “colds” are caused by an influenza virus. Presumably this number is about 55 million to get the widely quoted 0.1 percent (one in 1000) infection fatality rate for influenza. This is an example of the CDC’s estimates from https://www.cdc.gov/flu/about/burden/index.html:
Thus, the CDC estimates about 55 million of the annual over 660 million “cold” cases in the United States is caused by “influenza disease” or “influenza” or “flu,” presumably meaning cases caused by influenza viruses. This is probably less than ten percent of all “colds.” The CDC also estimates about 55,000 deaths from influenza viruses. This presumably gives the about 0.1 percent (one in 1000) number widely quoted in the media.
Everyone should understand that a 0.1 percent (one in 1000) infection fatality rate is much higher than the effective infection fatality rate of all the diseases that cause deaths attributed to “pneumonia and influenza” and that also typically cause two “common colds” or “flus” in healthy adults each year.
Even accepting the CDC’s estimates of the prevalence of illness due to influenza viruses (THE VIRUS), less than ten percent of all “common colds,” if the coronavirus COVID-19 spreads more easily than the influenza viruses, it may be able to kill more people than the influenza viruses with the same infection fatality rate (e.g. one in 1000, 0.1 percent). We also need to know how the SARS-COV-2 coronavirus spreads and how quickly.
If everyone in the United States were infected with the COVID-19 coronavirus, a 0.1 percent infection fatality rate (one in 1,000) would probably mean somewhat less than 330,000 additional deaths on top of the roughly 188,000 deaths from “pneumonia and influenza” (or is it 55,000 from “influenza and pneumonia”). There would be some overlap between COVID-19 coronavirus deaths and deaths of susceptible, mostly elderly persons that would have happened anyway due to conventional non-COVID diseases including the influenza viruses.
Conclusion
There is a remarkable lack of key measurements in the current coronavirus COVID-19 pandemic. These include the actual mortality rate (aka infection fatality rate) broken down by age, sex, race, pre-existing medical conditions, ambient temperature, sunlight levels, pollution levels, and other risk factors. The false positive and false negative rates of the tests for the disease, both the tests for an active infection such as the RT-PCR tests and tests for past infection such as the antibody tests. The methods and rates of transmission for the disease. Aerosol transmission probably occurs at least at a low level and is virtually unstoppable.
The CDC and the National Security bioweapons defense programs should have been set up to quickly and efficiently collect these key data and parameters as soon as a possible outbreak or attack was detected, independent of warnings and information provided by a potential adversary such as China or from the World Health Organization (WHO).
The confusing language and numbers on pneumonia and influenza on the CDC web site and in various official reports and documents seem to be primarily for marketing the flu vaccines rather than enabling informed decisions by patients and doctors or supporting external scientific research into the influenza viruses or other diseases.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
Addressing COVID-19 is a pressing health and social concern. To date, many epidemic projections and policies addressing COVID-19 have been designed without seroprevalence data to inform epidemic parameters. We measured the seroprevalence of antibodies to SARS-CoV-2 in Santa Clara County.
Methods
On 4/3-4/4, 2020, we tested county residents for antibodies to SARS-CoV-2 using a lateral flow immunoassay. Participants were recruited using Facebook ads targeting a representative sample of the county by demographic and geographic characteristics. We report the prevalence of antibodies to SARS-CoV-2 in a sample of 3,330 people, adjusting for zip code, sex, and race/ethnicity. We also adjust for test performance characteristics using 3 different estimates: (i) the test manufacturer’s data, (ii) a sample of 37 positive and 30 negative controls tested at Stanford, and (iii) a combination of both.
Results The unadjusted prevalence of antibodies to SARS-CoV-2 in Santa Clara County was 1.5% (exact binomial 95CI 1.11-1.97%), and the population-weighted prevalence was 2.81% (95CI 2.24-3.37%). Under the three scenarios for test performance characteristics, the population prevalence of COVID-19 in Santa Clara ranged from 2.49% (95CI 1.80-3.17%) to 4.16% (2.58-5.70%). These prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50-85-fold more than the number of confirmed cases.
Conclusions
The population prevalence of SARS-CoV-2 antibodies in Santa Clara County implies that the infection is much more widespread than indicated by the number of confirmed cases. Population prevalence estimates can now be used to calibrate epidemic and mortality projections.
This is of course a preliminary study.
It is worth noting that officially only about sixty (60) people have died of Coronavirus COVID-19 in Santa Clara County CA, a county of almost two million residents with very close ties to China. If true the preliminary study results would indicate that the actual mortality rate in Santa Clara County is well below one percent of those infected (60/48,000 is 0.125 percent for example).
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This is a video showing the CDC Cold vs Flu web page on April 16, 2020 shortly after I published my “Uncounted COVID Deaths? The CDC’s Contradictory Pneumonia and Influenza Death Numbers” where I discussed the contradictory language and claims on the CDC’s Cold vs Flu web page. The video was recorded to support further my discussion in the Uncounted COVID article/presentation and because I think it likely the web page will change as the CDC fields hard questions about its Influenza and Pneumonia web pages, reports, and other documentation.
Astonishingly the CDC gives two radically different numbers of deaths from pneumonia and influenza: about 55,000 “influenza and pneumonia” deaths in the leading causes of death table in the “Final Deaths” report for 2017, the latest year available, and about 188,000 in data on weekly “pneumonia and influenza” deaths, over THREE TIMES the leading causes of death number.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
An in-depth interview on the Coronavirus COVID-19 Pandemic and the proper response. Dr. Katz repeatedly notes the need for much better data on who has been or is infected and the actual mortality rate broken down by risk factors including age, sex, pre-existing medical conditions and so forth.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
I have added a video showing the CDC Pneumonia and Influenza Weekly Deaths web site as it is (was) on April 15, 2020. In this video I show the different web site sections I have discussed, download theNCHSData14.csvweekly deaths data file, go through the analysis briefly in a spreadsheet, and show the difference between the numbers in 2017 in the file and the Final Death (Leading Causes of Deaths) numbers in 2017.
The weekly pneumonia and influenza deaths data shows fewer deaths in weeks one through thirteen, the latest week in the file ending March 28, 2020, than in the comparable weeks in 2019 — last year. This despite the COVID-19 pandemic, lack of testing in the United States, asymptomatic carriers, and other issues.
The weekly pneumonia and influenza deaths data also show about 188,000 deaths from pneumonia and influenza in 2017, over THREE TIMES the about 55,000 deaths listed as “influenza and pneumonia” in the 2017 leading causes of death.
NOTE: If you are concerned about these odd numbers, please consider sharing the original post and/or this one by e-mail, a link on your web site or blog, or other methods in addition to advertising-funded and other big company social media. My original post of this on Hacker News soared for a few hours and then was flagged and shut down, for example. I have also encountered social media mobs that engage in name calling and do not address the substantive issues.
CDC Web Site Video
It seems likely to me that the CDC web site will change in response to questions about the confusing numbers and language. Hopefully, the CDC will clarify the language and numbers in an open, “transparent,” and genuinely honest way that survives critical scrutiny. Especially given the life and death situation.
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
This presentation discusses the CDC’s contradictory weekly and annual pneumonia and influenza deaths. Even the latest (as of April 14, 2020) weekly death numbers show fewer deaths in 2020 than comparable weeks last year (2019) despite the Coronavirus COVID-19 pandemic. Given asymptomatic carriers and inadequate testing in the United States, one would expect a surge in reported pneumonia and influenza deaths.
Remarkably summing the weekly pnemonia and influenza deaths gives about 180,000 annual deaths from pneumonia and influenza, over THREE TIMES the widely cited 55,000 “influenza and pneumonia” deaths from the annual leading causes of death report.
These numbers raise troubling questions about the CDC and its collection, analysis and reporting of pneumonia and influenza numbers. The low number of weekly deaths compared to last year could indicate that there may be many uncounted COVID deaths, or that the disease is much less deadly than popular reports, or several other possibilities with substantially different public health implications. The numbers need to be clarified as soon as possible.
Both a video version and a written PDF version are provided below. The written version is generally faster to read and includes references and some additional technical details.
NOTE: If you are concerned about these odd numbers, please consider sharing this post by e-mail, a link on your web site or blog, or other methods in addition to advertising-funded and other big company social media. My post of this on Hacker News soared for a few hours and then was flagged and shut down, for example. I have also encountered social media mobs that engage in name calling and do not address the substantive issues.
Video Presentation
Uncounted COVID Deaths? The CDC’s Contradictory Pneumonia and Influenza Death Numbers
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
As of March 21, 2020, the United States Centers for Disease Control (CDC) has posted weekly death numbers for pneumonia and influenza (P&I) that are substantially lower than the weekly death numbers for the matching weeks last year (2019) despite the Coronavirus COVID-19 Pandemic. This is remarkable given that with the lack of widespread testing many deaths caused by the pandemic would be expected to appear as a surge in deaths attributed to pneumonia and influenza. One can also argue that deaths caused by COVID-19, where known, should be included in the pneumonia and influenza death tally as well.
NOTE: The latest numbers, through the week ending March 21, 2020, were posted last Friday, April 3, 2020.
The weekly numbers for 2017 and previous years also sum to a total number of annual deaths due to pneumonia and influenza that is about three times larger than the widely quoted numbers from the 2017 and earlier leading causes of death reports.
I have done a number of video posts on the seeming absence of COVID-19 from reports through March 21, 2020. Remarkably the latest raw (?) data file NCHSData13.csv from https://www.cdc.gov/flu/weekly/#S2 (click on View Chart Data below the plot) shows total 40,002 deaths in week 12 of 2020 and 57,086 total deaths in week 12 of 2019 (see screenshot below) — much lower in 2020 despite the pandemic. The file shows total pneumonia and influenza deaths of 3,261 in week 12 of 2020 and 4,276 deaths in week 12 of 2019 (last year). Again many more deaths last year.
CDC Pneumonia and Influenza Deaths File NCHSData13.csv
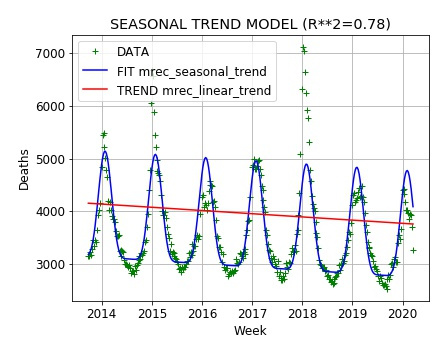
Remarkably the weekly death numbers attributed to pneumonia and influenza have been running below last year’s numbers for the same weeks for almost all weeks since the beginning of 2020 and well below what might be expected from simple modeling of the long term trend and seasonal variation.
In the plot below, the green plus signs are the data from the NCHSData13.csv file. The red line is the long term trend and the blue line if the full model with a roughly sinusoidal model of the seasonal variation in deaths added. One can see that the weekly death numbers are lower this year than last year and also fall well below the model prediction.
US Centers for Disease Control (CDC) Weekly Deaths from Pneumonia and Influenza (to March 21, 2020)
There are many possible explanations for this remarkable shortfall in deaths. No doubt the CDC is fielding hard questions from web site visitors, analysts, and others. Fox News host Tucker Carlson included the discrepancy in his commentary on the COVID-19 crisis on April 7 (from 3:24 to 3:50 in the linked video):
Tucker Carlson Highlights the CDC P and I Deaths Anomaly
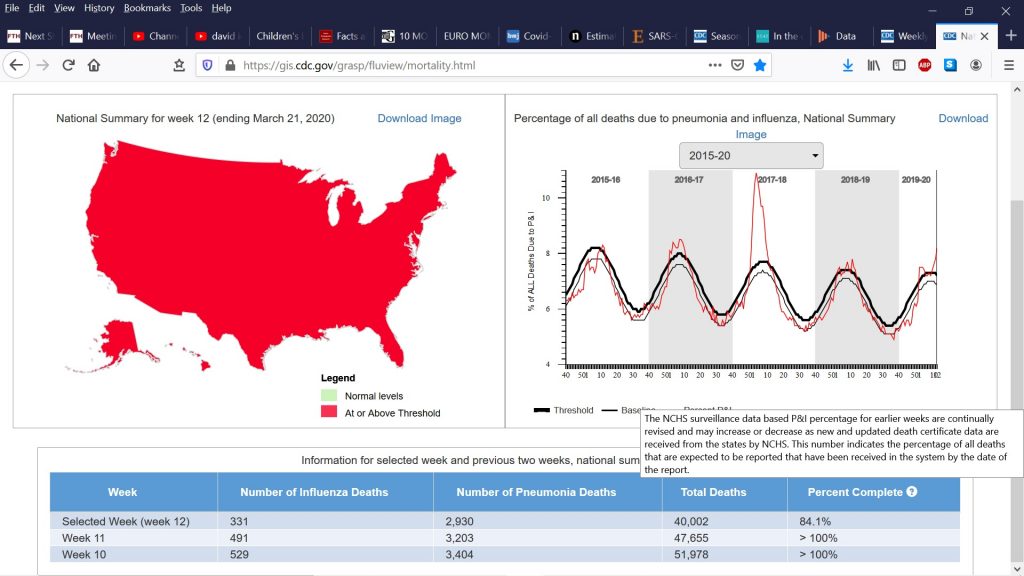
The CDC appears to have updated its FluView web site with information on how complete the numbers for the last three weeks are — how many death certificates have been collected. They appear to have added a table at the bottom with the weekly numbers:
CDC FluView Table on Pneumonia and Influenza Deaths (AT BOTTOM)
The final right-most column labeled “Percent Complete” seems to refer to how complete the numbers are, although this is not clear. Hovering the mouse pointer over the question mark to the right of “Percent Complete” brings up a legal disclaimer and not a clear explanation of what “Percent Complete” means. The final week (week 12, ending March 21, 2020) is listed as 85.4 % complete. Oddly, the previous two weeks (week 10 and week 11) are listed as (> 100 %) complete — note the greater than sign. Since one-hundred percent (100%) means COMPLETE, it is especially difficult to understand the use of the greater than sign > in the table. 🙂
In the FluView application/web page (today, April 9, 2020) the CDC seems to be claiming the numbers up to week 11 ending March 14, 2020 are in fact complete. The remarkable absence of COVID-19 deaths up to March 14, 2020 cannot be attributed to delays in collecting and processing death certificates or reports. A number of legal disclaimers such as the popup shown seem to have appeared recently (last few days) on the CDC web site.
As I have noted there are many possible explanations for this remarkable reported decline in deaths during a purported pandemic. It may be that people have been extra careful during the pandemic, staying home, avoiding risky behaviors, thus resulting in a drop in deaths both in general and from pneumonia and influenza causes other than COVID-19. It could be there are errors or omissions caused by the crisis response that are making the numbers unreliable. It could be pneumonia and influenza deaths from other causes are being incorrectly labeled as COVID-19 and omitted from the numbers; this is why it would be best to include COVID-19 as part of the P&I deaths. It could be that COVID-19, despite the headlines, is not unusually deadly.
NOTE: Total deaths in Europe have risen sharply in the latest weekly numbers from EuropMOMO, consistent with an unusually deadly new cause of death, after many weeks of remarkably showing no sign of the COVID-19 pandemic.
The CDC Weekly Pneumonia and Influenza Death Numbers are Three Times the Widely Reported Annual Death Numbers
Astonishingly the weekly death numbers in the NCHSData13.csv file — which go back to 2013 as shown in the plot above — indicate that about three times as many people in the United States have died from pneumonia and influenza in 2017 and preceding years as reported in the National Vital Statistics.
For example, the National Vital Statistics Report Volume 69, Number 8 dated June 24, 2019: “Deaths: Final Data for 2017” gives 55,672 deaths from “Influenza and pneumonia” in its table (Table B) of leading causes of deaths. “Influenza and pneumonia” is the eighth leading cause of death in 2017.
Death: Final Data for 2017Leading Causes of Death Table (2017)
Note that the report uses the phrase “Influenza and pneumonia” whereas the weekly death web site uses the language “Pneumonia and influenza (P&I)”. As I will explain below this may be a clue to the reason for the huge discrepancy.
In contrast, summing the weekly death numbers for 2017 in NCHSData13.csv gives 188,286 deaths for the entire year. This is OVER three times the number in the “Deaths: Final Data for 2017” (June 24, 2019).
It is worth noting that the web site, the NCHSData13.csv file, and the report appear intended for the general public, in part for educational and informational purposes — as well as doctors and other professionals who have limited time to dig into the numbers. Most people would interpret deaths due to “Influenza and pneumonia” in one report as the same or nearly the same (except for minor technical issues) number as “Pneumonia and influenza” in another report, data file, or web site.
What gives?
In 2005, Peter Doshi, an associate editor with the British Medical Journal (BMJ), one of the most prestigious medical journals in the world, wrote a highly critical, though short, article on the CDC’s pneumonia and influenza numbers: “Are US flu death figures more PR than science?”
BMJ. 2005 Dec 10; 331(7529): 1412. PMCID: PMC1309667
US data on influenza deaths are a mess. The Centers for Disease Control and Prevention (CDC) acknowledges a difference between flu death and flu associated death yet uses the terms interchangeably. Additionally, there are significant statistical incompatibilities between official estimates and national vital statistics data. Compounding these problems is a marketing of fear—a CDC communications strategy in which medical experts “predict dire outcomes” during flu seasons.
The CDC website states what has become commonly accepted and widely reported in the lay and scientific press: annually “about 36 000 [Americans] die from flu” (www.cdc.gov/flu/about/disease.htm) and “influenza/pneumonia” is the seventh leading cause of death in the United States (www.cdc.gov/nchs/fastats/lcod.htm). But why are flu and pneumonia bundled together? Is the relationship so strong or unique to warrant characterising them as a single cause of death?
BMJ. 2005 Dec 10; 331(7529): 1412. PMCID: PMC1309667
Peter Doshi goes on in this vein for a couple of pages (see the linked article above). Peter Doshi and other sources online seem to suggest that CDC estimates a large number of pneumonia deaths that are attributed to secondary effects of influenza such as a bacterial pneumonia infection caused by influenza. Influenza is rarely detected in actual tests of actual patients and only a small fraction of deaths reported in the weekly statistics are attributed in NCHSData13.csv to influenza (the virus, NOT “flu” as used in popular language which can mean any disease with similar symptoms to influenza — the scientific term).
The influenza and pneumonia deaths number in the National Vital Statistics Report may be this estimate that Doshi is describing in his critical article in the BMJ. The other (many more!) weekly “pneumonia and influenza” deaths presumably are assigned to some other categories in the annual leading causes of death report.
Presumably CDC can give some explanation for this vast discrepancy between two numbers that most of us would expect to be the same. “Influenza and pneumonia” and “pneumonia and influenza” mean the same thing in common English usage. They almost certainly mean the same thing to most doctors and other health professionals as well.
Conclusion
These pneumonia and influenza death numbers need to be clarified in an open and transparent manner. The next set of numbers will probably be posted tomorrow Friday April 10, 2020. Hopefully these new numbers and accompanying commentary will explain the situation in an open and transparent manner that survives critical scrutiny.
The proper response to the COVID-19 pandemic depends on knowing a range of parameters including the actual mortality rate broken down by age, sex, race, obesity, other medical conditions, whatever can be measured quickly and accurately. The actual rates and modes of transmission. The false positive and false negative rates for the various tests, both for active infection and past infection. These are mostly not known.
Most of us are experiencing the instinctive fight or flight response which degrades higher cognitive function, aggravated by the 24/7 Internet/social media fear barrage. It is important to calm down, collect actual data in a genuinely open, transparent way that will yield broad public support, and think carefully.
UPDATE (February 13, 2021):
We have received some questions about more up to date information on the issues raised in this article. Our most recent and comprehensive article on the CDC’s historical influenza and pneumonia death numbers and their current COVID-19 death numbers is:
This article argues that the US Centers for Disease Control (CDC)’s April 2020 guidance for filling out death certificates for possible COVID-19 related deaths strongly encourages, if not requires, assigning COVID-19 as the underlying cause of death (UCOD) in any death where COVID-19 or the SARS-COV-2 virus may be present, which appears to differ from common historical practice for pneumonia and influenza deaths where pneumonia was frequently treated as a “complication,” a cause of death but not the underlying cause of death.
This means the number of COVID deaths should be compared to a count of death certificates where pneumonia and influenza were listed as a cause of death or even a lesser contributing factor, a historical number which appears to have been at least 188,000 per year based on the CDC FluView web site. The proper comparison number may be even larger if deaths that historically were listed as heart attacks, cancer or other causes than pneumonia or influenza are also being reassigned due to the April 2020 guidance.
Here are some earlier articles and references:
This is a more recent article/video on the long standing problems with the pneumonia and influenza death numbers:
“How Reliable are the US Centers for Disease Control’s Death Numbers” (October 14, 2020)
The second article on the Santa Clara County death numbers includes a detailed section on the changes in the standard on assigning the underlying cause of death for COVID cases from the CDC’s April 2020 “guidance” document, which probably boost the COVID death numbers substantially. This section is broken out and edited into this article:
We are looking at the CDC’s excess death numbers which appear to be highly questionable. The CDC follows a non-standard procedure of zeroing out data points that are negative in summing the excess deaths. See this article by Tam Hunt:
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).
The luxury apartment project across the street from where I live has paused in the Coronavirus COVID-19 Pandemic. I thank those responsible and briefly discuss the proper steps to deal with the pandemic based on knowledge and data rather than fear and panic.
(C) 2020 by John F. McGowan, Ph.D.
About Me
John F. McGowan, Ph.D. solves problems using mathematics and mathematical software, including developing gesture recognition for touch devices, video compression and speech recognition technologies. He has extensive experience developing software in C, C++, MATLAB, Python, Visual Basic and many other programming languages. He has been a Visiting Scholar at HP Labs developing computer vision algorithms and software for mobile devices. He has worked as a contractor at NASA Ames Research Center involved in the research and development of image and video processing algorithms and technology. He has published articles on the origin and evolution of life, the exploration of Mars (anticipating the discovery of methane on Mars), and cheap access to space. He has a Ph.D. in physics from the University of Illinois at Urbana-Champaign and a B.S. in physics from the California Institute of Technology (Caltech).